Pretibial myxedema
Pretibial myxedema is a cutaneous manifestation of autoimmune thyroid disease, most commonly seen in Graves’ disease. It is a form of localized dermopathy caused by accumulation of glycosaminoglycans (hyaluronic acid, chondroitin sulfate) in the dermis and subcutaneous tissue.
🔹 Key Features
- Location: Usually on the anterior aspect of the tibia (pretibial area), but can also occur on feet, ankles, and dorsum of hands.
- Appearance:
- Localized, firm, non-pitting edema
- Skin appears shiny, waxy, and thickened
- Orange-peel (peau d’orange) texture due to prominent hair follicles
- Color may be pink, violaceous, or brownish
- Symmetry: Usually bilateral, but can be asymmetric.
- Symptoms: Usually painless, but may cause cosmetic concerns, itching, or discomfort.
🔹 Pathophysiology
- Caused by autoimmune stimulation of fibroblasts by TSH receptor–stimulating antibodies (the same antibodies responsible for hyperthyroidism in Graves’ disease).
- Fibroblasts produce excess glycosaminoglycans, leading to dermal thickening and edema.
🔹 Clinical Associations
Pretibial myxedema is part of the extra-thyroidal manifestations of Graves’ disease, which include:
- Graves’ ophthalmopathy (thyroid eye disease)
- Acropachy (clubbing with periosteal bone formation)
- Pretibial myxedema
This triad is sometimes called the EMO syndrome (Exophthalmos, Myxedema, Osteoarthropathy).
🔹 Diagnosis
- Clinical appearance is usually diagnostic.
- Thyroid function tests confirm associated thyrotoxicosis.
- Biopsy (rarely needed) shows mucin deposition in dermis.
🔹 Management
Most cases are mild and self-limiting.
- General measures: Compression stockings, emollients.
- Topical therapy: High-potency topical corticosteroids under occlusion.
- Systemic therapy: Rarely needed; immunosuppressive therapy (rituximab, teprotumumab, etc.) used in severe cases.
- Treat underlying Graves’ disease, though skin findings may persist even after correction of thyroid function.
✅ Key Point for Exams (USMLE/PG):
Pretibial myxedema is pathognomonic for Graves’ disease and presents as non-pitting, shiny, peau d’orange thickening of the skin over the shins, caused by TSH receptor antibodies stimulating fibroblasts.
Pretibial Myxedema — 20 MCQs
Q1. Which of the following is the classic dermatologic appearance of pretibial myxedema?
Answer: A. Pretibial myxedema shows firm, non-pitting, waxy thickening with an orange-peel (peau-d’orange) appearance over the shins.
Q2. Pretibial myxedema is most commonly associated with which thyroid disorder?
Answer: B. Pretibial myxedema is an extra-thyroidal manifestation of Graves’ disease and is strongly associated with TSH-receptor antibodies.
Q3. The primary dermal substance that accumulates in pretibial myxedema is:
Answer: C. Fibroblasts produce excess glycosaminoglycans (mainly hyaluronic acid), leading to mucinous dermal edema and thickening.
Q4. Which antibody is primarily implicated in the pathogenesis of pretibial myxedema?
Answer: D. TSH-receptor stimulating antibodies (TRAb) stimulate dermal fibroblasts to produce glycosaminoglycans and inflammatory mediators.
Q5. Which of the following extracutaneous features commonly coexists with pretibial myxedema?
Answer: A. Pretibial myxedema often coexists with Graves’ ophthalmopathy; both are autoimmune reactions mediated by TRAb and shared antigenic targets in orbital and dermal fibroblasts.
Q6. The texture “peau d’orange” in pretibial myxedema refers to:
Answer: B. The peau d’orange appearance is dimpling of the skin produced by expansion of dermal tissue around hair follicles and is characteristic of mucin deposition conditions.
Q7. Which histologic finding is typical on biopsy of pretibial myxedema?
Answer: C. Biopsy reveals abundant mucopolysaccharide (mucin) in the dermis and subcutis, often with increased fibroblasts; inflammation may be mild.
Q8. First-line topical therapy for localized, symptomatic pretibial myxedema is:
Answer: D. High-potency topical corticosteroids under occlusion are commonly used for localized lesions and often provide symptomatic and cosmetic improvement.
Q9. Which statement about the natural history of pretibial myxedema is true?
Answer: A. Skin changes can persist even after euthyroidism is achieved because the autoimmune process in fibroblasts may continue independently of circulating thyroid hormone levels.
Q10. Which systemic therapy has shown benefit in severe, refractory pretibial myxedema in case series and small studies?
Answer: B. Intralesional corticosteroids, systemic steroids for severe disease, and immunomodulatory therapies (eg, rituximab) have been used for refractory cases.
Q11. Thyroid acropachy (clubbing & periosteal reaction) is most closely associated with which of the following?
Answer: C. Thyroid acropachy is a rare manifestation that typically occurs with severe Graves’ disease and often coexists with eye disease and pretibial myxedema.
Q12. Which non-invasive measure may provide symptomatic improvement for mild pretibial myxedema?
Answer: D. Supportive measures—compression, elevation, and emollients—can help symptomatic mild cases and improve cosmesis in some patients.
Q13. Which of the following is NOT a typical location for pretibial myxedema?
Answer: A. Classic locations are the anterior shins; it can also affect dorsum of feet, ankles, or rarely other sites—palms are not typical.
Q14. Which imaging or lab finding is most useful to confirm underlying Graves’ disease in a patient with pretibial myxedema?
Answer: B. TRAb positivity along with thyroid function tests (low TSH, elevated T4/T3) supports diagnosis of Graves’ disease associated with pretibial myxedema.
Q15. Which of the following best describes why pretibial myxedema is non-pitting?
Answer: C. Accumulated mucin (GAGs) and fibroblast proliferation trap fluid in the dermis, making the swelling firm and non-pitting.
Q16. Which of the following newer targeted therapies has been reported to improve severe thyroid eye disease and may indirectly relate to extra-thyroidal manifestations?
Answer: D. Teprotumumab, an IGF-1R monoclonal antibody, has shown benefit for thyroid eye disease; modulation of autoimmune pathways may impact other manifestations, though direct benefit on pretibial myxedema is less established.
Q17. In clinical practice, biopsy of pretibial myxedema is:
Answer: A. Diagnosis is usually clinical; biopsy is reserved for atypical presentations or when ruling out other dermatoses.
Q18. Which patient education point is appropriate for someone with pretibial myxedema?
Answer: B. Management includes controlling Graves’ disease; however, cutaneous changes can persist and may require local therapy or specialist referral.
Q19. Which specialist is most appropriate to involve for refractory or severe pretibial myxedema?
Answer: C. Dermatology input for local and systemic dermatologic treatments is appropriate; endocrinology manages the underlying thyroid disease—multidisciplinary care is common.
Q20. Which of the following best summarizes the pathophysiology of pretibial myxedema?
Answer: D. The autoimmune process (TSH-receptor antibodies) stimulates fibroblasts to produce glycosaminoglycans leading to mucin deposition, inflammation, and dermal thickening.
Tip: Answers are revealed on first click. Use Reset buttons to try again.
| Feature | Description |
|---|---|
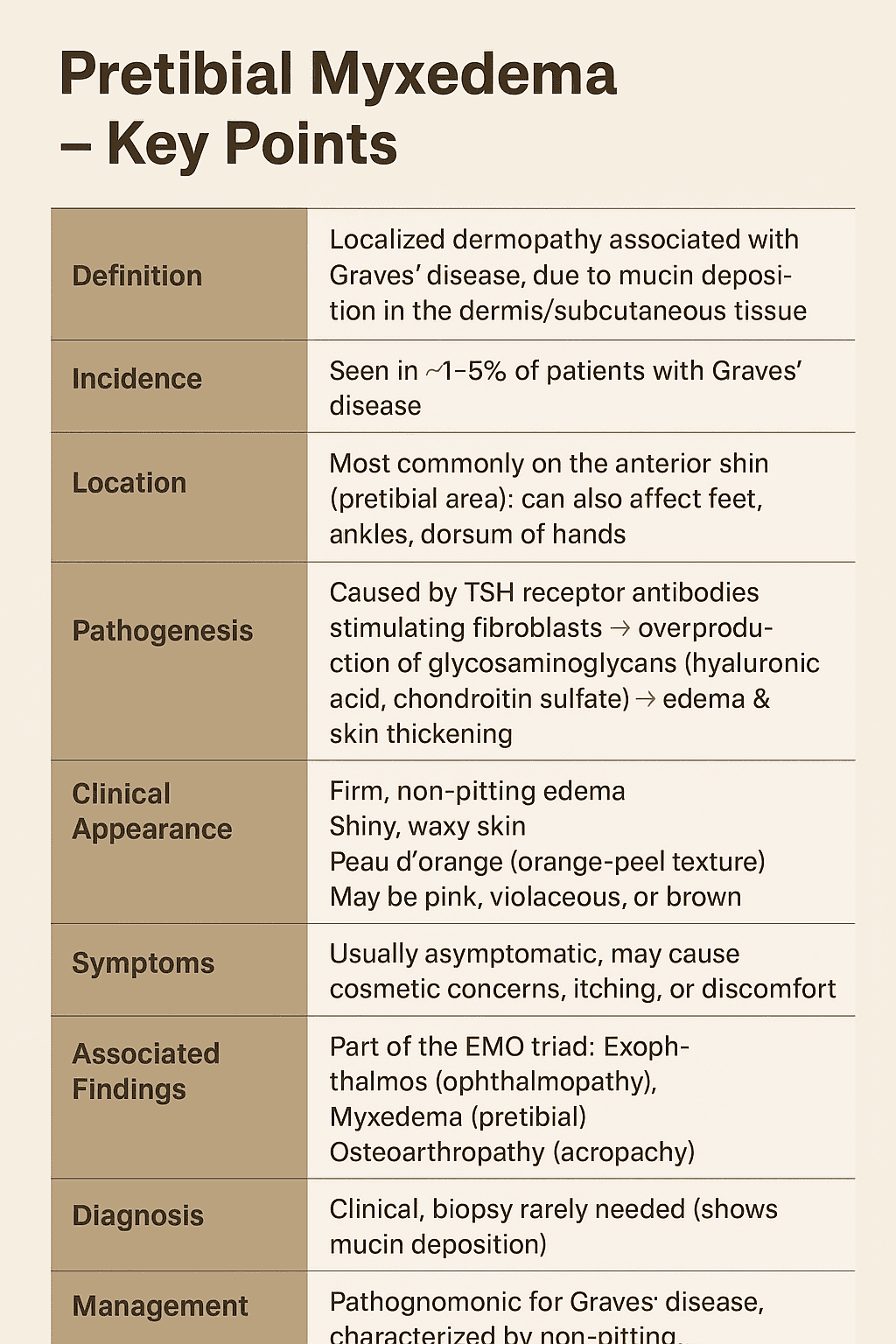
| Definition | Localized dermopathy associated with Graves’ disease, due to mucin deposition in the dermis/subcutaneous tissue. |
| Incidence | Seen in ~1–5% of patients with Graves’ disease. |
| Location | Most commonly on the anterior shin (pretibial area); can also affect feet, ankles, dorsum of hands. |
| Pathogenesis | Caused by TSH receptor antibodies stimulating fibroblasts → overproduction of glycosaminoglycans (hyaluronic acid, chondroitin sulfate) → edema & skin thickening. |
| Clinical Appearance | – Firm, non-pitting edema – Shiny, waxy skin – Peau d’orange (orange-peel texture) – May be pink, violaceous, or brown. |
| Symptoms | Usually asymptomatic; may cause cosmetic concerns, itching, or discomfort. |
| Associated Findings | Part of the EMO triad: – Exophthalmos (ophthalmopathy) – Myxedema (pretibial) – Osteoarthropathy (acropachy). |
| Diagnosis | Clinical; biopsy rarely needed (shows mucin deposition). |
| Management | – General: Compression stockings, emollients – Topical: High-potency corticosteroids (under occlusion) – Systemic: Rare; immunomodulators in severe cases – Treat underlying Graves’ disease. |
| Key Exam Point | Pathognomonic for Graves’ disease, characterized by non-pitting, peau d’orange thickening over shins. |
Pretibial myxedema is a localized lesions of the skin resulting from the deposition of
- [A] Fluid
- [B] Hyaluronic acid
- [C] beta-2 microglobulin
- [D] Transthyretin
All of the following are TRUE for Pretibial myxedema EXCEPT
- [A] almost always preceded by the ocular signs found in Graves’ disease
- [B] peau d’orange (orange peel) appearance
- [C] non-pitting edema of the skin
- [D] biopsy of the affected skin commonly reveals increase in fibroblasts
Pretibial myxedema
- Nearly always associated with autoimmune thyroid disease – Graves Disease
- Most often confined to the pretibial area, it may occur anywhere on the skin, especially the ankle, dorsum of the foot, knees, shoulders, elbows, upper back, pinnae, nose, and neck