1. The SYNTAX score primarily quantifies which of the following?
A. Anatomical complexity of coronary artery disease
B. Myocardial viability
C. Left ventricular ejection fraction
D. Degree of ischemia on stress testing
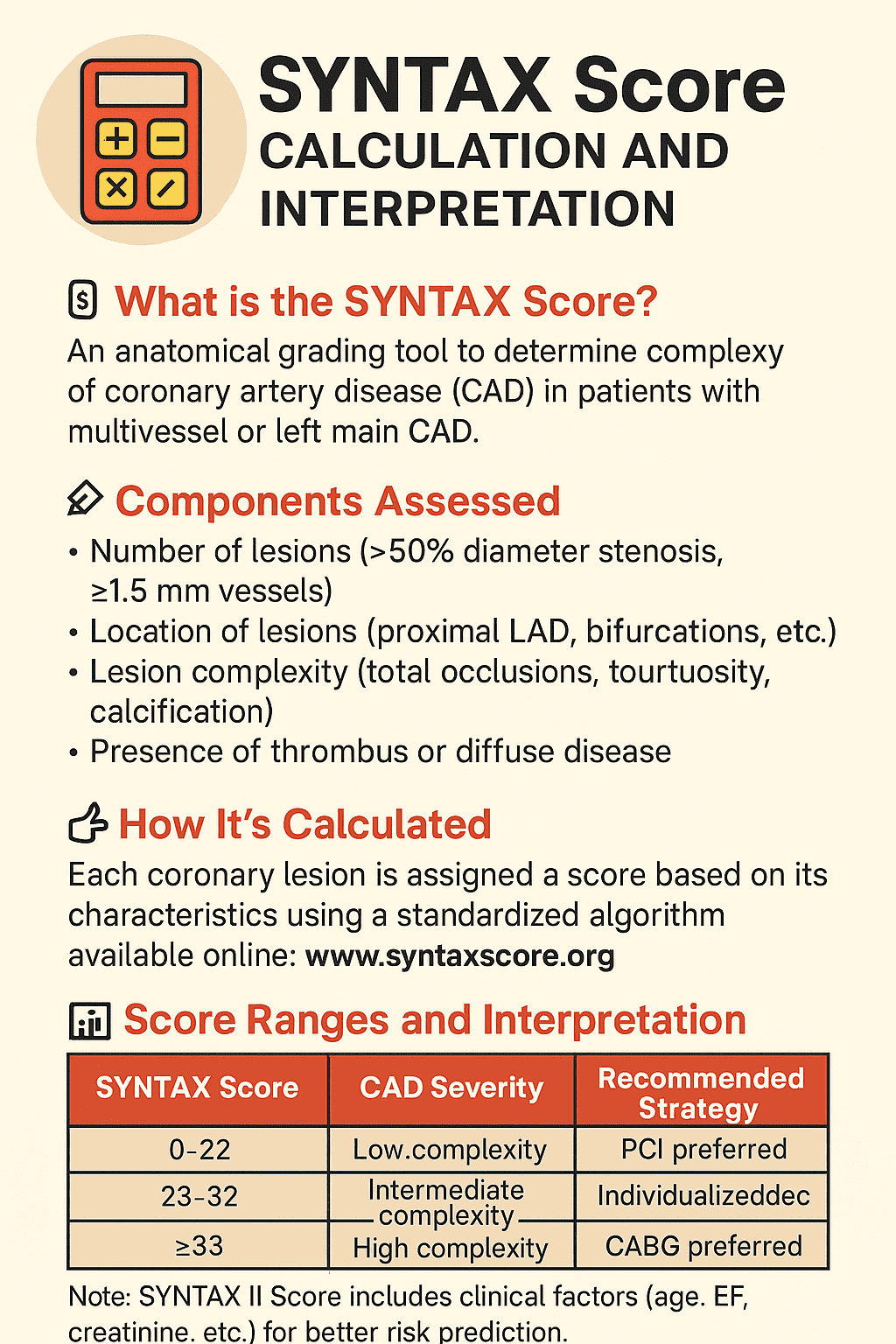
SYNTAX is an angiographic (anatomic) score measuring lesion complexity (bifurcations, total occlusions, calcification, etc.).
2. The original SYNTAX score was developed from data of patients enrolled in which treatment comparison?
A. PCI vs medical therapy
B. PCI (with DES) vs CABG
C. CABG vs medical therapy
D. PCI vs thrombolysis
The SYNTAX score arose from analysis of patients in trials comparing PCI (drug-eluting stents) with CABG for complex CAD.
3. Which lesion feature is scored in the SYNTAX calculation?
A. Degree of angina
B. Exercise tolerance
C. Bifurcation involvement
D. Serum cholesterol level
SYNTAX scores lesion-level anatomical features — bifurcation involvement increases the complexity score.
4. A commonly used SYNTAX score threshold that defines “high” anatomical complexity is:
A. ≤22
B. 23–32
C. 20–25
D. ≥33
SYNTAX categories: low (≤22), intermediate (23–32), and high (≥33) — high scores indicate complex disease favoring CABG.
5. Which of these increases the SYNTAX score for an individual lesion?
A. Chronic total occlusion
B. History of MI
C. Low-density lipoprotein level
D. Prior stroke
Chronic total occlusion is explicitly scored and increases SYNTAX complexity.
6. In clinical decision-making, a high SYNTAX score generally favors which revascularization strategy?
A. Percutaneous coronary intervention (PCI)
B. Coronary artery bypass grafting (CABG)
C. Medical therapy alone
D. Thrombolysis
High SYNTAX (≥33) was associated with better outcomes after CABG than PCI in trials, so CABG is usually preferred.
7. Which of the following is NOT directly part of the anatomical SYNTAX score calculation?
A. Lesion length
B. Vessel dominance
C. Patient age
D. Presence of tortuosity
Patient age is a clinical variable (used in SYNTAX II), but not in the original anatomical SYNTAX calculation.
8. SYNTAX II score differs from SYNTAX I by adding:
A. Additional lesion morphological parameters only
B. Imaging-based plaque composition
C. Procedural technical details
D. Clinical variables (e.g., age, LVEF, creatinine)
SYNTAX II integrates clinical factors (age, gender, LVEF, creatinine, COPD, peripheral vascular disease) with anatomy to guide decision-making.
9. Which coronary segment involvement often contributes disproportionately to the SYNTAX score due to myocardial territory at risk?
A. Left main or proximal LAD lesions
B. Distal small-caliber branches
C. Small posterolateral branches
D. Coronary veins
Proximal left main or proximal LAD lesions are weighted heavily because they jeopardize large myocardial territories.
10. Which procedural or lesion characteristic reduces the ease of percutaneous treatment and increases SYNTAX score?
A. Short focal lesion
B. Severe calcification
C. Single non-bifurcation lesion
D. Straight vessel without tortuosity
Severe calcification complicates PCI (stent expansion) and therefore raises the anatomical complexity score.
11. How is the SYNTAX score typically calculated in practice?
A. By bedside clinical scoring only
B. From ECG and biomarkers
C. Using an angiographic lesion-based algorithm (often with online/software tool)
D. From stress imaging
Operators map each lesion on angiography and use the SYNTAX algorithm or validated calculator to compute the score.
12. Which statement about SYNTAX score is TRUE?
A. It predicts only stroke risk
B. It is identical to the Gensini score
C. It is based solely on clinical comorbidities
D. It quantifies anatomical complexity and helps guide revascularization strategy
SYNTAX is an angiographic tool to quantify complexity and assist choice between PCI and CABG when combined with clinical judgment.
13. In a patient with 3-vessel disease and SYNTAX score of 18, what is the usual interpretation?
A. Low anatomical complexity — PCI may be reasonable
B. High complexity — CABG is mandatory
C. Syntax does not apply to 3-vessel disease
D. Immediate medical therapy only
A score ≤22 is considered low; for multivessel disease with low SYNTAX, PCI outcomes may be comparable to CABG in selected patients.
14. Which of the following is a limitation of the SYNTAX score?
A. It integrates left ventricular function automatically
B. It does not capture several important clinical variables (without SYNTAX II)
C. It was designed for non-coronary vascular disease
D. It is validated only for valve disease
SYNTAX I is purely anatomical; important clinical factors (age, LVEF, creatinine) are not included unless using SYNTAX II.
15. Which anatomical finding commonly scored in SYNTAX indicates increased technical difficulty during PCI?
A. Superficial plaque only
B. Focal ostial lesion without branching
C. Severe vessel tortuosity
D. Single small distal lesion in a tiny branch
Severe tortuosity complicates guidewire/catheter passage and is assigned points in SYNTAX.
16. For which patient group is SYNTAX scoring most commonly applied clinically?
A. Patients with arrhythmias only
B. Those with isolated non-calcified single-vessel disease
C. Patients undergoing stress tests only
D. Patients with complex multivessel or left main coronary artery disease being considered for revascularization
SYNTAX is particularly useful when choosing between CABG and PCI for multivessel or left main disease.
17. Which of the following changes would LOWER a patient’s SYNTAX score?
A. Treating/rewiring a small side branch so the lesion is not scored as a separate complex bifurcation (i.e., reclassifying anatomy)
B. Adding another chronic total occlusion
C. Documenting severe calcification
D. Identifying additional long lesions
SYNTAX reflects the angiographic anatomy — if anatomy is reassessed and complexity reduced (fewer scored lesions), the score falls.
18. A SYNTAX score can help predict which long-term outcome difference between PCI and CABG?
A. Valve durability
B. Need for repeat revascularization (higher after PCI with higher SYNTAX)
C. Incidence of pneumonia
D. Incidence of peripheral arterial disease
Higher SYNTAX correlates with higher repeat revascularization rates after PCI compared with CABG in complex disease.
19. Which clinical variable is specifically included in the SYNTAX II algorithm but NOT SYNTAX I?
A. Lesion length
B. Bifurcation status
C. Left ventricular ejection fraction (LVEF)
D. Vessel tortuosity
SYNTAX II adds clinical predictors such as LVEF, age, creatinine clearance, etc., to the anatomical score.
20. Which practical step is recommended when a heart team evaluates a patient with multivessel disease?
A. Use only clinical judgment without anatomy
B. Randomly choose PCI or CABG
C. Always perform PCI regardless of complexity
D. Integrate SYNTAX (anatomic) score with clinical factors and discuss in a heart team to choose PCI vs CABG
Best practice: combine anatomical scoring (SYNTAX) with clinical variables (SYNTAX II) and multidisciplinary heart-team discussion to individualize revascularization.
Therefore, “Syntax >50% diameter vessel size >” indicates that the report is describing a coronary lesion that is significant (causing more than 50% narrowing) and located in a major vessel (larger than 1.5 mm in diameter) that will be included in the calculation of the overall SYNTAX score.
In essence, “Syntax >50% diameter vessel size >” in a medical report would be interpreted as a significant finding, indicating a significant blockage in a major coronary artery that contributes to the patient’s overall SYNTAX score and risk assessment.