Risk stratification and management of unstable angina and NSTEMI
Risk Stratification and Management of Unstable Angina (UA) and NSTEMI, integrating scores, biomarkers, ECG, imaging, and invasive strategy timing.
Unstable Angina & NSTEMI
Risk Stratification and Management
1. Definitions (Exam Clarity)
| Feature | Unstable Angina (UA) | NSTEMI |
|---|---|---|
| Troponin | Negative | Positive |
| ECG | ST depression / T inversion / normal | Same |
| Pathology | Subtotal occlusion, platelet-rich thrombus | Subtotal occlusion ± microembolization |
| Management | Similar initially | Similar but more aggressive invasive strategy |
UA is becoming rare due to high-sensitivity troponins detecting NSTEMI.
2. Initial Risk Stratification – Core Pillars
A. Clinical Risk Features (High-risk clues)
- Recurrent or ongoing chest pain
- Hemodynamic instability / shock
- Acute heart failure
- Malignant arrhythmias
- Mechanical complications
- Post-PCI or post-CABG angina
B. ECG Risk Stratification
| ECG Finding | Risk |
|---|---|
| ST depression ≥0.5 mm | High |
| Dynamic ST-T changes | High |
| T-wave inversion ≥1 mm in ≥2 leads | Intermediate |
| Normal ECG | Low (NOT benign) |
ST depression = NSTEMI until proven otherwise
C. Biomarkers
- High-sensitivity troponin (hs-cTn)
- Rising/falling pattern = myocardial infarction
- Magnitude correlates with mortality
- BNP / NT-proBNP → prognostic, not diagnostic
3. Formal Risk Scores (Very Important)
1️⃣ GRACE Score (MOST IMPORTANT)
Predicts in-hospital and 6-month mortality
Variables:
- Age
- HR
- SBP
- Creatinine
- Killip class
- Cardiac arrest
- ST deviation
- Troponin elevation
| GRACE Score | Risk Category | Strategy |
|---|---|---|
| >140 | High | Early invasive (<24 h) |
| 109–140 | Intermediate | Invasive within 24–72 h |
| <109 | Low | Conservative / selective |
GRACE >140 = guideline trigger for <24 h angiography
2️⃣ TIMI Risk Score (Older but exam-favorite)
1 point each:
- Age ≥65
- ≥3 CAD risk factors
- Known CAD (>50%)
- Aspirin use in last 7 days
- ≥2 angina episodes in 24 h
- ST deviation ≥0.5 mm
- Positive troponin
| TIMI | Risk |
|---|---|
| 0–2 | Low |
| 3–4 | Intermediate |
| 5–7 | High |
3️⃣ CRUSADE Score (Bleeding Risk)
Used to:
- Adjust anticoagulation
- Decide access (radial preferred)
- Balance ischemia vs bleeding
4. Management Strategy (Stepwise)
A. Immediate Management (ALL Patients)
1️⃣ Anti-Ischemic Therapy
- Oxygen only if SpO₂ <90%
- Nitrates (SL → IV if ongoing pain)
- Beta-blockers (unless shock, asthma, AV block)
- Morphine → only if refractory pain
2️⃣ Antiplatelet Therapy
Aspirin
- Loading: 150–300 mg
- Maintenance: 75–100 mg lifelong
P2Y12 Inhibitor (Choose carefully)
| Drug | Use |
|---|---|
| Clopidogrel | Conservative or unknown anatomy |
| Ticagrelor | Preferred in invasive strategy |
| Prasugrel | Only after angiography |
Never preload prasugrel before anatomy known
3️⃣ Anticoagulation
| Setting | Preferred |
|---|---|
| Conservative | Fondaparinux |
| Invasive | UFH / Enoxaparin |
| PCI | UFH ± GP IIb/IIIa (bailout) |
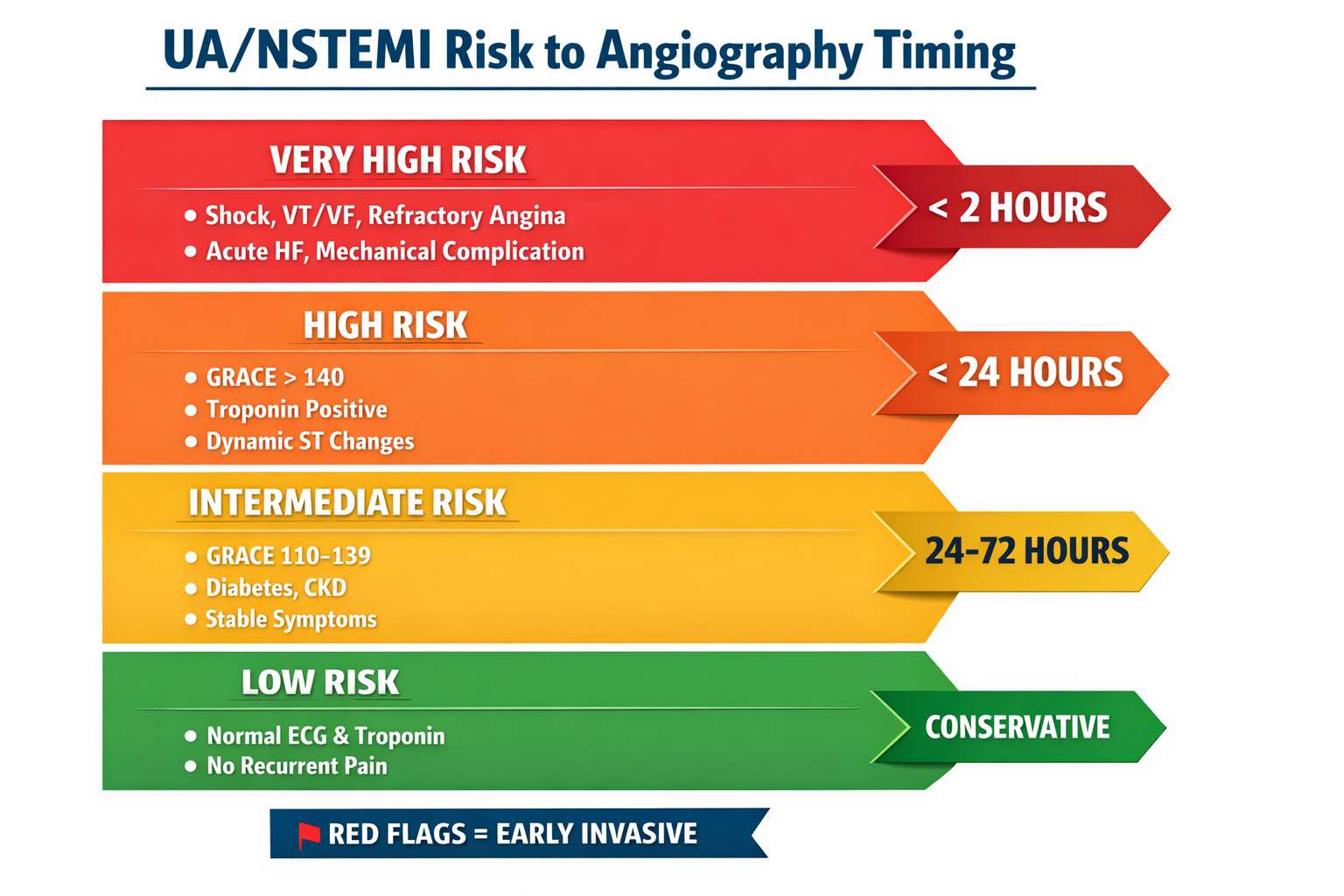
B. Risk-Based Invasive Strategy (KEY EXAM AREA)
Timing of Coronary Angiography
| Strategy | Indication |
|---|---|
| Immediate (<2 h) | Shock, refractory angina, life-threatening arrhythmia |
| Early (<24 h) | GRACE >140, ↑ troponin, dynamic ST changes |
| Delayed (24–72 h) | Diabetes, renal dysfunction, EF <40% |
| Conservative | Low-risk, stable, normal troponin |
5. Revascularization Decision
PCI
- Focal culprit lesion
- Ongoing ischemia
- High-risk anatomy
CABG
- Left main disease
- Multivessel + diabetes
- Complex anatomy (high SYNTAX)
6. Secondary Prevention (Before Discharge)
Mandatory Medications
- DAPT (12 months unless bleeding)
- High-intensity statin
- Beta-blocker
- ACEI / ARB
- MRA if EF ≤40% + HF/DM
Lifestyle
- Smoking cessation
- Cardiac rehab
- BP, sugar, lipid control
7. High-Yield Exam Pearls
- GRACE >140 = <24 h angiography
- NSTEMI ≠ STEMI but mortality similar
- UA = troponin negative only
- Fondaparinux → add UFH during PCI
- Radial access ↓ bleeding
- Prasugrel only AFTER coronary anatomy
1. A NSTEMI patient has GRACE score 152, stable vitals, troponin rising, no ongoing pain. Best timing of angiography?
Immediate (<2 hours)
Early (<24 hours)
Delayed (24–72 hours)
Conservative only
GRACE >140 mandates **early invasive strategy <24 h**, not immediate unless instability.
2. Which variable is NOT part of the GRACE risk score?
Serum creatinine
Killip class
Diabetes mellitus
ST-segment deviation
Diabetes influences risk but **is not a GRACE variable**.
3. UA has become rare in the hs-troponin era primarily because:
Less plaque rupture
Minor necrosis is now detected as NSTEMI
Improved ECG sensitivity
More conservative definitions
High-sensitivity troponins reclassify many UA cases as NSTEMI.
4. Best anticoagulant strategy in NSTEMI planned for conservative management?
Fondaparinux
Bivalirudin
UFH only
No anticoagulation
Fondaparinux provides best ischemic–bleeding balance in conservative strategy.
5. A patient on fondaparinux undergoes PCI. What is mandatory?
Switch to LMWH
Add UFH during PCI
Stop anticoagulation
Add GP IIb/IIIa upfront
Fondaparinux alone causes **catheter thrombosis** → UFH is mandatory during PCI.
6. Which scenario mandates IMMEDIATE (<2 h) angiography in NSTEMI?
Refractory angina despite therapy
Troponin rise only
Diabetes mellitus
EF 38%
Refractory ischemia = **very-high-risk** → immediate invasive strategy.
7. Prasugrel in NSTEMI should be started:
At first medical contact
With aspirin in ER
Only after coronary anatomy is known
Only after PCI
Pre-treatment with prasugrel increases bleeding—**never before angiography**.
8. CRUSADE score is primarily used to predict:
Mortality
In-hospital bleeding
Reinfarction
Heart failure
CRUSADE helps tailor antithrombotic intensity and access site.
9. ST depression ≥0.5 mm in NSTEMI implies:
High-risk ischemia
Low-risk ACS
Posterior STEMI only
Troponin-negative ACS
ST depression is a **powerful adverse prognostic marker**.
10. Which trial showed benefit of early invasive strategy in high-risk NSTEMI?
TIMACS
COURAGE
ISCHEMIA
FAME-2
TIMACS: **GRACE >140 subgroup benefited from <24 h angiography**.
11. In NSTEMI, which subgroup derived mortality benefit from early (<24 h) invasive strategy in TIMACS trial?
All NSTEMI patients
GRACE score >140
Troponin-negative UA
Diabetics only
TIMACS showed benefit of early strategy **only in high-risk (GRACE >140)** patients.
12. A stable NSTEMI patient with troponin rise but normal ECG belongs to which risk category?
Low risk
High risk
Very high risk
No-risk ACS
**Troponin positivity alone = high risk**, even with normal ECG.
13. Which factor upgrades NSTEMI to “very high risk” requiring <2 h angiography?
Hemodynamic instability
GRACE 145
Positive troponin
Diabetes mellitus
Shock, refractory angina, malignant arrhythmia = **very high risk**.
14. Which antiplatelet strategy is preferred if coronary anatomy is unknown?
Aspirin + ticagrelor
Aspirin + prasugrel
Prasugrel monotherapy
Triple therapy upfront
Prasugrel is **contraindicated before anatomy is known**.
15. Which anticoagulant has the lowest bleeding risk in NSTEMI?
Fondaparinux
UFH
Enoxaparin
Bivalirudin
Fondaparinux shows **best net clinical benefit** (OASIS-5).
16. NSTEMI patient with GRACE 110, stable, diabetic. Best angiography timing?
<2 h
<24 h
24–72 h
Conservative only
Intermediate risk + diabetes → **delayed invasive (24–72 h)**.
17. Which ECG change carries the worst prognosis in NSTEMI?
Diffuse ST depression with aVR elevation
Isolated T-wave inversion
Normal ECG
Sinus tachycardia
ST depression + aVR elevation suggests **LM / severe multivessel disease**.
18. Which trial showed reduced ischemic events but increased bleeding with routine GP IIb/IIIa use?
EARLY-ACS
TIMACS
OASIS-5
ACUITY
EARLY-ACS → **no routine upstream GP IIb/IIIa**.
19. Radial access in NSTEMI primarily reduces:
Bleeding and mortality
Contrast volume
Procedure time
Stent thrombosis
Radial access → **lower bleeding = mortality benefit**.
20. NSTEMI with severe anemia and CRUSADE high risk—best approach?
Bleeding-avoidance strategy
Aggressive triple therapy
Delay all antithrombotics
Fibrinolysis
CRUSADE guides **bleeding-risk mitigation**, not ischemia denial.
21. Which feature differentiates NSTEMI from unstable angina?
Troponin elevation
ST depression
Chest pain at rest
Plaque rupture
**Troponin positivity defines MI**, not ECG or symptoms.
22. Which NSTEMI patient can be managed conservatively?
Normal troponin, normal ECG, stable
Troponin positive
Dynamic ST changes
GRACE 145
Low-risk ACS → ischemia-guided strategy acceptable.
23. Which drug should be avoided in acute NSTEMI with shock?
Beta-blocker
Aspirin
Heparin
Statin
Beta-blockers worsen shock—**contraindicated acutely**.
24. NSTEMI + LVEF 35% + multivessel disease—preferred revascularization?
CABG
Culprit-only PCI
Medical therapy
Deferred angiography
LV dysfunction + multivessel disease → **CABG favored**.
25. Which biomarker adds prognostic but not diagnostic value in NSTEMI?
NT-proBNP
Troponin
CK-MB
Myoglobin
BNP predicts HF/mortality, **not MI diagnosis**.
26. Which scenario favors ticagrelor over clopidogrel?
Planned early invasive strategy
High bleeding risk
Oral anticoagulation needed
Severe bradycardia
Ticagrelor preferred in **invasive NSTEMI**, unless bleeding risk high.
27. NSTEMI patient develops VT—risk category?
Very high risk
High risk
Intermediate risk
Low risk
Life-threatening arrhythmia = **immediate invasive indication**.
28. Why is fibrinolysis contraindicated in NSTEMI?
No benefit and increased bleeding
Lack of thrombus
Always complete occlusion
Causes reinfarction
NSTEMI has **non-occlusive thrombus** → fibrinolysis harmful.
29. Most common cause of death in NSTEMI?
Pump failure
Arrhythmia
Free wall rupture
Stroke
NSTEMI mortality is driven by **LV dysfunction and HF**.
30. Which NSTEMI subset has mortality comparable to STEMI?
High-risk NSTEMI
Troponin-negative UA
Low-risk NSTEMI
Post-PCI NSTEMI
High-risk NSTEMI has **similar or worse long-term mortality**.
31. NSTEMI with CKD—best contrast-minimizing strategy?
Radial access + hydration
Delay angiography indefinitely
Avoid revascularization
High-dose contrast bolus
CKD is **not a contraindication**—optimize technique.
32. NSTEMI + AF on DOAC—preferred antiplatelet?
Clopidogrel
Ticagrelor
Prasugrel
Triple DAPT
Clopidogrel minimizes bleeding in **dual therapy with OAC**.
33. NSTEMI patient with severe AS—key concern?
Hypotension with nitrates
Statin intolerance
Troponin false positivity
Bleeding risk
Fixed outflow obstruction → **nitrates can cause collapse**.
34. Best marker of reinfarction after NSTEMI?
CK-MB
hs-Troponin
Myoglobin
BNP
CK-MB normalizes faster → useful for **reinfarction detection**.
35. NSTEMI patient with prior CABG—angiography timing?
Early invasive
Conservative
Always delayed
No angiography
Post-CABG ACS is **high risk**.
36. NSTEMI with isolated troponin rise after tachyarrhythmia is termed?
Type 2 MI
Unstable angina
Type 1 MI
Myocarditis
Supply–demand mismatch = **Type 2 MI**.
37. Which NSTEMI patient benefits MOST from statins?
All patients irrespective of LDL
Only LDL >190
Diabetics only
Post-PCI only
High-intensity statin is **Class I for all ACS**.
38. NSTEMI + mechanical complication—strategy?
Immediate invasive + surgery
Medical therapy
Delayed angiography
Fibrinolysis
Mechanical complications = **very high risk ACS**.
39. NSTEMI patient discharged on DAPT—minimum duration?
12 months
1 month
6 months
Lifelong
Standard ACS DAPT = **12 months**, unless bleeding.
40. NSTEMI mortality is reduced most by:
Risk-based invasive strategy
Routine fibrinolysis
Morphine
Routine GP IIb/IIIa
Correct **risk stratification + invasive timing saves lives**.
Risk Stratification & Management of UA/NSTEMI — exam-grade, memory-anchoring, no fluff.
🧠 UA / NSTEMI — 50 Ultra-Hard One-Liners (NEET-SS Final Week)
- GRACE >140 = angiography <24 h, not immediate unless unstable.
- Very-high-risk NSTEMI = <2 h angiography, irrespective of GRACE.
- Troponin positivity alone upgrades ACS to high risk, even with normal ECG.
- UA is defined only by negative troponin, not by ECG or symptoms.
- hs-Troponin has nearly eliminated true UA in modern practice.
- Diffuse ST depression with aVR elevation = LM / severe 3-vessel disease.
- ST depression is prognostically worse than isolated T-wave inversion.
- TIMACS benefit of early strategy was confined to GRACE >140.
- EARLY-ACS killed routine upstream GP IIb/IIIa use.
- Fondaparinux causes catheter thrombosis unless UFH is added during PCI.
- Fondaparinux has the best ischemia–bleeding balance in NSTEMI.
- CRUSADE predicts bleeding, not ischemic risk.
- High CRUSADE ≠ no antithrombotics; it means bleeding-avoidance strategy.
- Radial access reduces mortality via bleeding reduction.
- Prasugrel is contraindicated before coronary anatomy is known.
- Ticagrelor is preferred when early invasive strategy is planned.
- Clopidogrel is preferred with oral anticoagulation.
- Fibrinolysis is contraindicated in NSTEMI due to harm without benefit.
- NSTEMI long-term mortality can exceed STEMI in high-risk subsets.
- Pump failure is the most common cause of death in NSTEMI.
- Beta-blockers are contraindicated in acute NSTEMI with shock.
- Nitrates can precipitate collapse in severe aortic stenosis.
- CK-MB is superior to troponin for diagnosing reinfarction.
- Post-CABG ACS is automatically high risk.
- Diabetes shifts NSTEMI from intermediate to delayed-invasive (24–72 h).
- Normal ECG does not imply low-risk NSTEMI.
- Life-threatening arrhythmia = very-high-risk ACS.
- Mechanical complications mandate immediate invasive + surgery.
- BNP adds prognostic, not diagnostic, value in NSTEMI.
- NSTEMI with tachyarrhythmia-induced troponin rise = Type 2 MI.
- Type 2 MI does not mandate routine invasive strategy.
- Oxygen is indicated only if SpO₂ <90%.
- Morphine increases adverse outcomes—use only for refractory pain.
- NSTEMI is usually due to subtotal, not complete, coronary occlusion.
- Early invasive strategy reduces recurrent ischemia, not always mortality.
- Delayed invasive = 24–72 h, not “watchful waiting.”
- Low-risk ACS = normal ECG + negative troponin + no recurrent pain.
- Statins are Class I in ACS irrespective of LDL level.
- CABG is preferred in NSTEMI with LV dysfunction + multivessel disease.
- NSTEMI + CKD is not a contraindication to angiography.
- Contrast nephropathy prevention = hydration + contrast minimization.
- aVR elevation in NSTEMI is a surgical red flag.
- Troponin magnitude correlates with mortality, not infarct size alone.
- NSTEMI with heart failure = high-risk ACS even without ST changes.
- Routine triple therapy is never default in NSTEMI.
- Early invasive strategy benefits ischemic outcomes most in high-risk patients.
- NSTEMI with ongoing pain despite therapy = immediate angiography.
- DAPT duration after NSTEMI is 12 months unless bleeding risk dominates.
- Risk stratification, not troponin alone, determines invasive timing.
- In NSTEMI, correct timing of angiography saves more lives than any single drug.







