Chiari network
Chiari network
Q1. The Chiari network is a remnant of which embryological structure?
Correct: C. The Chiari network is a persistent, fenestrated remnant of the right valve of the sinus venosus.
Q2. Which imaging modality most clearly visualizes the Chiari network?
Correct: A. TEE provides high-resolution images of the right atrium, allowing clear visualization of thin, mobile Chiari network filaments.
Q3. The Chiari network is most commonly found in which chamber?
Correct: B. It is located in the right atrium, near the junction of the IVC and coronary sinus.
Q4. Typical echocardiographic appearance of the Chiari network is:
Correct: D. The Chiari network is thin, highly mobile, and filamentous, often moving independently of the tricuspid valve.
Q5. What is the approximate prevalence of the Chiari network on routine echocardiography?
Correct: C. It is rare on routine echocardiography, observed in about 0.3–1.5% of patients.
Q6. Which of the following is a potential clinical implication of the Chiari network?
Correct: A. The Chiari network can direct flow towards a PFO, facilitating paradoxical embolism.
Q7. How does the Chiari network differ from a right atrial thrombus?
Correct: B. Unlike thrombus, the Chiari network is highly mobile and web-like, with filamentous appearance.
Q8. Which association is commonly reported with the Chiari network?
Correct: C. PFO is often associated, which may increase risk of paradoxical embolism.
Q9. The Chiari network may complicate which of the following procedures?
Correct: D. Its mobile filaments can entangle pacemaker or central venous catheters.
Q10. Most Chiari networks require which treatment?
Correct: B. They are mostly benign and do not require intervention unless associated complications occur.
Q11. The Chiari network arises due to incomplete regression of which valve?
Correct: A. It is a remnant of the right valve of the sinus venosus.
Q12. On echocardiography, Chiari network motion is typically:
Correct: C. It moves independently within the right atrium, often freely with blood flow.
Q13. Which of these can mimic the Chiari network?
Correct: B. Right atrial thrombus can appear similar but is denser, less mobile, and broad-based.
Q14. The Chiari network is best described as:
Correct: D. Its classic feature is a fenestrated, net-like, web-like appearance.
Q15. Chiari network incidence is higher in:
Correct: A. Autopsy series show higher incidence due to more detailed examination.
Q16. Which clinical condition may prompt intervention for Chiari network?
Correct: C. Intervention is rarely required, mainly for complications like paradoxical embolism or device entanglement.
Q17. Chiari network may influence which of the following?
Correct: B. It can alter flow within the right atrium, especially towards a PFO.
Q18. Which statement is TRUE regarding Chiari network?
Correct: C. Most cases are incidental and do not cause hemodynamic compromise.
Q19. Chiari network may coexist with which atrial structure?
Correct: D. Chiari network is often associated with Eustachian valve remnants.
Q20. What is the main reason to differentiate Chiari network from thrombus?
Correct: B. Thrombus requires treatment; Chiari network usually does not.
Q21. Chiari network may complicate which procedure the most?
Correct: A. Its filaments can entangle leads during pacemaker placement or central venous catheterization.
Q22. Which echocardiographic clue suggests Chiari network rather than thrombus?
Correct: C. Thin, mobile, net-like filaments favor Chiari network.
Q23. Chiari network may increase risk of:
Correct: B. Flow directed towards a PFO may facilitate paradoxical emboli.
Q24. Most Chiari networks are discovered:
Correct: D. They are usually found incidentally on TTE or TEE.
Q25. Which part of the RA is Chiari network typically attached to?
Correct: A. Typically along IVC–coronary sinus junction.
Q26. Chiari network may simulate which rare right atrial pathology?
Correct: C. Its appearance can mimic RA thrombus, but mobility and texture help differentiate.
Q27. Which statement about Chiari network management is TRUE?
Correct: B. Most Chiari networks are benign; intervention only if complications occur.
Q28. Which imaging feature helps distinguish Chiari network from tricuspid valve leaflet?
Correct: C. Chiari network moves independently and is filamentous, unlike valve leaflets.
Q29. Which is NOT a typical feature of Chiari network?
Correct: D. RA enlargement is not typical; Chiari network is usually benign and small.
Q30. Key clinical pearl regarding Chiari network:
Correct: A. It is mostly incidental, but awareness is important for device placement and embolic risk.
Chiari network. Let me give you a structured, clear explanation:
🔹 Chiari Network — Overview
- The Chiari network is a fenestrated, net-like embryologic remnant found in the right atrium of the heart.
- First described by Hans Chiari in 1897.
- It is usually benign and incidental, but clinically relevant in some scenarios.
🔹 Anatomy
- Located in the right atrium, near the junction of the inferior vena cava (IVC) and the coronary sinus ostium.
- Originates from incomplete regression of the right valve of the sinus venosus during embryonic development.
- Appears as a thin, mobile, filamentous structure (like a “spider web”) on echocardiography.
🔹 Incidence
- Seen in ~2–4% of autopsies.
- Found in 0.3–1.3% of echocardiographic studies.
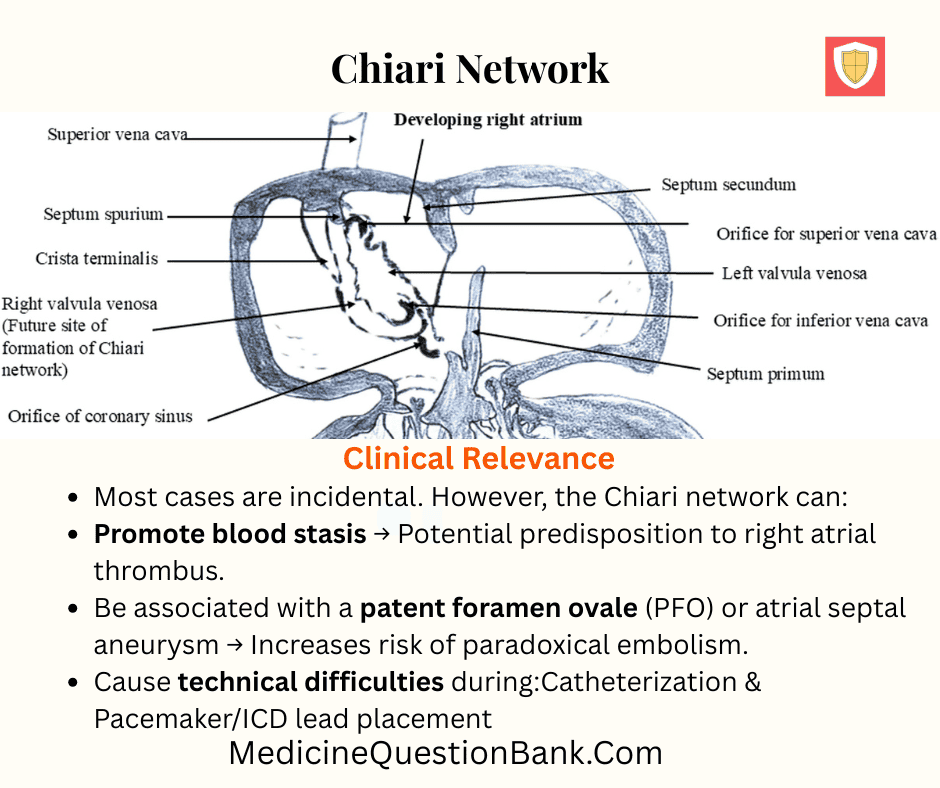
🔹 Clinical Relevance
Most cases are incidental. However, the Chiari network can:
- Promote blood stasis → Potential predisposition to right atrial thrombus.
- Be associated with a patent foramen ovale (PFO) or atrial septal aneurysm → Increases risk of paradoxical embolism.
- Cause technical difficulties during:
- Catheterization
- Pacemaker/ICD lead placement
- Right heart interventions
- Rarely, may act as a nidus for infective endocarditis.
- Sometimes confused with:
- Thrombus
- Vegetation
- Flail tricuspid chordae
🔹 Echocardiographic Features
- Seen as a highly mobile, reticulated structure in the right atrium.
- Best visualized on TEE (transesophageal echo).
- Key point: Moves independently of the tricuspid valve leaflets, helping differentiate from other pathology.
🔹 Associations
- Patent foramen ovale (PFO)
- Atrial septal aneurysm
- Persistent Eustachian valve
- Paradoxical embolism / stroke
🔹 Clinical Pearls
- Usually benign and requires no treatment.
- Important to recognize to avoid misdiagnosis (esp. as RA thrombus or vegetation).
- If associated with PFO + paradoxical embolism, may influence closure decisions.
Chiari network
Which embryologic structure is the Chiari network derived from?
Answer: A. The Chiari network represents incomplete regression of the right valve of the sinus venosus (the embryologic Eustachian valve region).
Where is the Chiari network most commonly seen?
Answer: C. The Chiari network is typically located in the right atrium at the junction of the IVC and coronary sinus ostium.
Approximate echocardiographic incidence of the Chiari network?
Answer: B. Reported prevalence on echo series is low — roughly 0.3–1.5%; autopsy series may be a bit higher.
Which best describes the echocardiographic appearance of the Chiari network?
Answer: D. On echo it is a mobile, reticulated, spider-web like structure distinct from fixed masses.
Which imaging modality most reliably visualizes the Chiari network?
Answer: A. TEE provides superior visualization of thin, mobile right atrial structures including the Chiari network.
The Chiari network is most commonly associated with which other intracardiac finding?
Answer: B. There is a known association between Chiari network and PFO, possibly due to embryologic persistence in the region.
Which statement about the Chiari network is TRUE?
Answer: C. Most Chiari networks are incidental and benign but can complicate procedures or be implicated in embolic events.
Which of the following is an important differential diagnosis when a mobile structure is seen in the right atrium?
Answer: D. Right atrial thrombus or vegetations must be distinguished from a Chiari network clinically and on echo.
How might the Chiari network theoretically contribute to paradoxical embolism?
Answer: A. The Chiari network can direct venous flow toward the atrial septum and PFO, facilitating paradoxical emboli.
Which procedural complication is the Chiari network known to potentially cause?
Answer: B. Its filamentous nature can entangle pacemaker leads or catheters and complicate right-sided procedures.
Which echo clue helps distinguish Chiari network from tricuspid valve tissue?
Answer: C. Chiari network moves independently of tricuspid leaflets, indicating it’s not valve tissue.
Is the Chiari network a common site for infective endocarditis?
Answer: D. Endocarditis involving Chiari network is rare but has been reported when organisms colonize mobile structures.
What is the typical management for an incidental Chiari network found on echo with no complications?
Answer: A. Incidental, asymptomatic Chiari networks usually require no intervention beyond clinical follow-up.
Which finding makes thrombus more likely than Chiari network?
Answer: B. Thrombi are often dense, immobile or less mobile and have a heterogeneous texture compared to Chiari network.
Color Doppler over the Chiari network typically shows:
Answer: C. Chiari network itself doesn’t have intrinsic flow; Doppler shows normal venous flow around it.
Which condition increases the risk of paradoxical embolism in presence of Chiari network?
Answer: D. A PFO or other interatrial communication allows right-to-left passage of thrombi redirected by the network.
Compared to echo series, autopsy studies report the Chiari network prevalence as:
Answer: A. Autopsy series may show higher prevalence because small networks may be missed on transthoracic echo.
Which physical exam finding is typically present with an isolated Chiari network?
Answer: B. Isolated Chiari network is usually silent on clinical exam; findings derive from associated lesions if present.
Which historical eponym is associated with the Chiari network?
Answer: C. The structure is named after Hans Chiari who described it in the late 19th century.
In pacemaker implantation complicated by Chiari network, the most appropriate next step is:
Answer: D. Careful technique and imaging (TEE/fluoroscopy) or alternative tools are preferred rather than force which risks damage.
The Chiari network is typically:
Answer: A. It’s characteristically thin and web-like rather than a bulky mass.
Chiari network presence is protective against pulmonary embolism because it traps thrombi in the right atrium. True or false?
Answer: B. Some case reports suggest entrapment of thrombi, but this doesn’t reliably protect from PE; clinical data are mixed.
The persistent Eustachian valve is most closely related to which structure?
Answer: C. Both are embryologic remnants of right-sided sinus venosus structures (Eustachian valve and Chiari network).
When is surgical excision of the Chiari network indicated?
Answer: D. Surgery is very uncommon and reserved for symptomatic or complicated cases not controllable by other measures.
Which ECG finding is typical for an isolated Chiari network?
Answer: A. Chiari network itself does not produce specific ECG changes; ECG changes suggest other pathology.
On transthoracic echo, what feature can falsely mimic a Chiari network?
Answer: B. Prominent crista terminalis or a large Eustachian valve may be confused with Chiari network on limited views.
Which rare complication has been described in case reports involving Chiari network?
Answer: C. Case reports document thrombus entrapment and paradoxical emboli when PFO coexists with Chiari network.
Presence of Chiari network influences decision for PFO closure in which way?
Answer: D. Chiari network is one factor among many; it may raise concern about embolic risk and factor into multidisciplinary decisions about PFO closure.
Recommended follow-up for an asymptomatic patient with Chiari network and no PFO?
Answer: A. Observation is appropriate; targeted follow-up if symptoms, thromboembolic events, or procedural plans arise.
Which succinct statement best summarizes the Chiari network?
Answer: B. It is an embryologic remnant of the right atrium, typically benign but important in certain clinical contexts.
| Chiari Network — Quick Clinical Infographic | |
|---|---|
| Definition | A net-like, reticulated embryologic remnant from incomplete regression of the right valve of the sinus venosus, often visualized near the IVC/coronary sinus junction. |
| Incidence | Rare on routine echocardiography (~0.3–1.5%), somewhat higher in autopsy series. Mostly incidental finding. |
| Anatomy & Embryology | Originates from the right sinus venosus valve (related to the Eustachian valve). Located in the right atrium near the IVC and coronary sinus ostium. |
| Echo Features | Thin, highly mobile, filamentous, web-like structure; moves independently of tricuspid leaflets; best seen on TEE or focused TTE views. |
| Clinical Tip | Tip Differentiate from RA thrombus (thrombus → denser, broad-based, less mobile) and vegetations. Consider associated PFO in embolic presentations. |
| Key Associations | PFO • Eustachian valve • Atrial septal aneurysm |
| Clinical Pearls |
|







