Post-PCI DAPT Summary (Clinician-Level)
Post-PCI DAPT Summary (Clinician-Level)
1. Core Components
DAPT = Aspirin + P2Y12 inhibitor
P2Y12 inhibitor choices:
- Ticagrelor 90 mg BID
- Prasugrel 10 mg daily (5 mg in patients <60 kg or >75 years)
- Clopidogrel 75 mg daily (when ticagrelor/prasugrel contraindicated)
Aspirin: 75–100 mg/day long-term.
2. Standard DAPT Duration After PCI
A. Acute Coronary Syndrome (ACS: STEMI/NSTE-ACS)
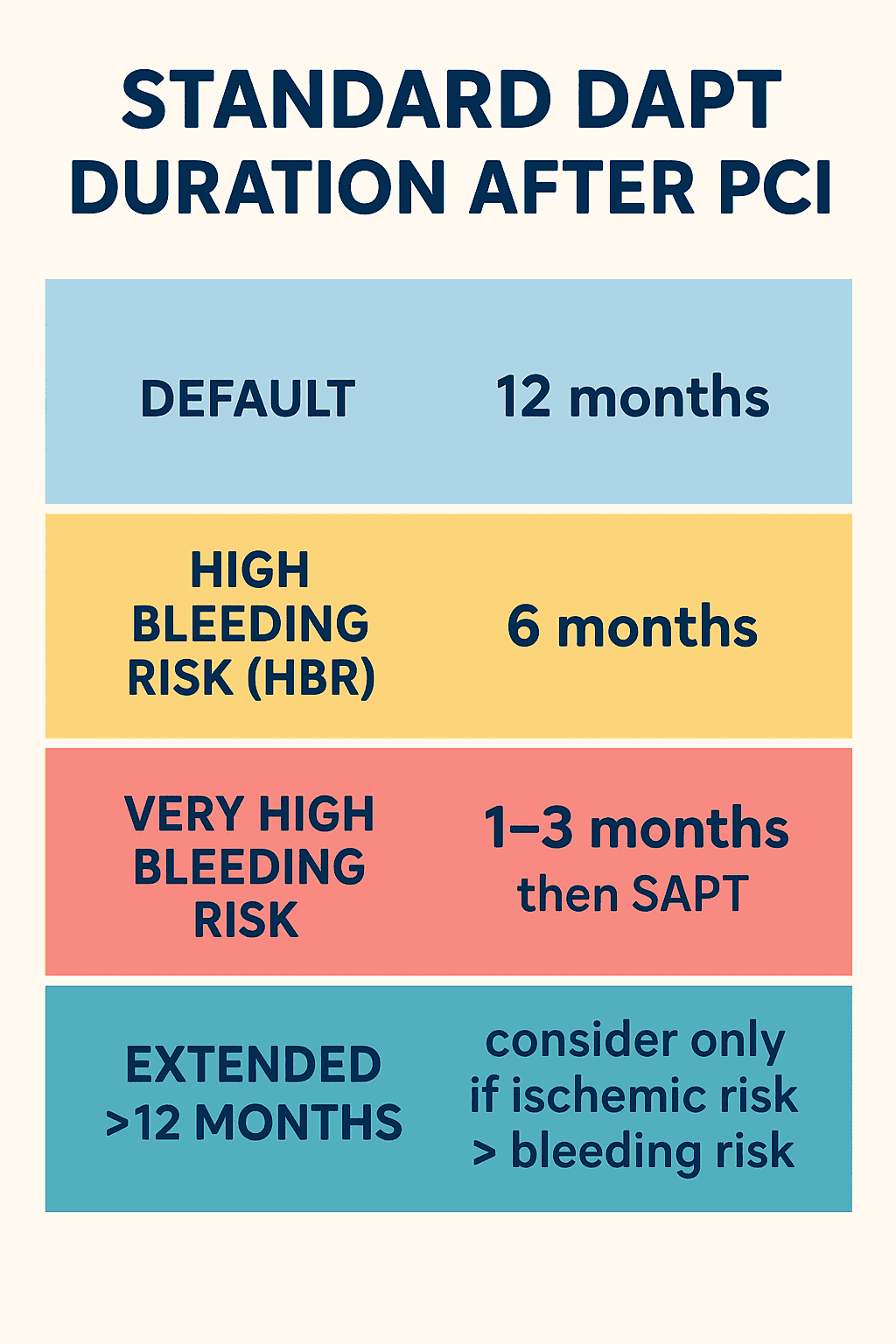
- Default: 12 months
- High bleeding risk (HBR): 6 months
- Very high bleeding risk: 1–3 months then SAPT
- Extended >12 months: consider only if ischemic risk > bleeding risk.
B. Stable Ischemic Heart Disease (SIHD)
- Default: 6 months
- High bleeding risk: 3 months
- Very high bleeding risk: 1 month then aspirin alone or P2Y12 monotherapy.
3. Choosing the P2Y12 Inhibitor (ACS)
- Preferred: Ticagrelor or Prasugrel
- Prasugrel avoided in: prior stroke/TIA, age >75 years (unless high thrombotic risk), weight <60 kg
- Clopidogrel if: cost issues, bleeding risk high, bradyarrhythmias, dyspnea with ticagrelor.
4. Post-PCI Special Situations
A. High Bleeding Risk (HBR)
Examples:
- Prior GI bleed, CKD, anemia, anticoagulant therapy, thrombocytopenia, OAC indication.
Management:
- Prefer short DAPT (1–3 months) then SAPT (clopidogrel or aspirin).
B. Complex PCI
(Stent length >60 mm, >3 stents, bifurcation with 2 stents, CTO, left main PCI)
- Consider intensified therapy (12–30 months) if bleeding risk low.
- Use prasugrel/ticagrelor unless contraindicated.
C. Patients on Oral Anticoagulants (AF + PCI)
- Triple therapy (Aspirin + clopidogrel + OAC): 1 week–1 month
- Then Dual therapy (OAC + clopidogrel) up to 6–12 months
- Then OAC alone.
5. DAPT Score for Extended Therapy
Used after 12 months event-free period post-PCI to decide if prolonged DAPT is beneficial.
- Score ≥2: Benefit > risk → consider extending DAPT
- Score <2: Stop DAPT → aspirin alone
Post‑PCI DAPT — 40 Advanced MCQs (Interactive)
Post‑PCI DAPT — 40 Frequently Asked Questions
- Default recommendation: 12 months for patients treated after ACS (STEMI/NSTE‑ACS).
- For stable ischemic heart disease (elective PCI): typically 6 months.
- Shorten to 3–6 months or even 1 month in high/very high bleeding risk as appropriate.
- Decisions individualized using patient ischemic vs bleeding risk balance.
- Reassess at 12 months with DAPT score before considering extension.
- Ticagrelor (90 mg BID) or prasugrel (10 mg daily) are preferred over clopidogrel for ACS when bleeding risk is acceptable.
- Prasugrel contraindicated with prior stroke/TIA and used cautiously in age >75 or weight <60 kg (dose reduction considered).
- Ticagrelor may cause dyspnea and bradyarrhythmia—switch if intolerant.
- Clopidogrel used when ticagrelor/prasugrel contraindicated or unavailable and when bleeding risk is higher.
- Choice should factor drug–drug interactions, adherence, cost, and CYP2C19 genotype if known.
- Default shorten DAPT to 3–6 months (HBR) or 1–3 months for very high bleeding risk.
- Prefer clopidogrel or P2Y12 monotherapy after short DAPT if aspirin discontinuation planned.
- Use ARC‑HBR criteria to formalize bleeding risk assessment.
- Consider vascular protection measures: PPI for GI risk, treat anemia, manage anticoagulants carefully.
- Document shared decision‑making and plan for close follow‑up.
- Consider extension only if ischemic risk substantially exceeds bleeding risk (eg prior MI, multivessel disease, complex PCI, low EF).
- Use DAPT score (calculated at 12 months event‑free) — score ≥2 favors extension.
- Extended therapy options include continuing original P2Y12 or switching to lower‑dose ticagrelor (eg 60 mg BD) for secondary prevention.
- Regularly reassess for bleeding events and drug tolerance during extension.
- Discuss benefits and bleeding trade‑offs with the patient before prolonging therapy.
- Minimize triple therapy (aspirin + P2Y12 + OAC); if used, keep duration short (often 1–7 days) then stop aspirin.
- Transition to dual therapy: OAC + clopidogrel (preferred) for up to 6–12 months depending on ischemic risk.
- Direct oral anticoagulants (DOACs) preferred over VKAs when appropriate, using guideline dosing.
- After 6–12 months, continue OAC alone for stroke prevention unless strong ischemic indication persists.
- Coordinate with cardiology and electrophysiology/hematology for individualized strategy.
- Calculated at 12 months in patients event‑free to guide extension of DAPT beyond 12 months.
- Scores ≥2 suggest ischemic benefit from extended DAPT; lower scores favor stopping P2Y12.
- Includes clinical variables (age, diabetes, prior MI/PCI, smoking, CHF/LVEF, stent characteristics).
- It is a decision aid — integrate with bleeding risk assessment (ARC‑HBR) and clinical judgment.
- Not validated for all populations; use cautiously in elderly and those on OACs.
- STOPDAPT‑2: 1‑month DAPT followed by clopidogrel monotherapy in selected patients.
- GLOBAL LEADERS and SMART‑CHOICE evaluated aspirin‑free or shorter strategies with mixed results.
- TWILIGHT tested early aspirin withdrawal with ticagrelor monotherapy in high‑risk patients showing reduced bleeding.
- Several trials support tailored shorter DAPT in modern DES era with careful patient selection.
- Apply trial findings selectively; consider local practice, stent type, and patient risk profiles.
- ARC‑HBR (Academic Research Consortium for HBR) defines major and minor bleeding risk criteria to standardize HBR identification.
- Major criteria include recent major bleed, severe anemia, long‑term OAC, severe CKD, thrombocytopenia, etc.
- Presence of ≥1 major or ≥2 minor criteria identifies HBR and supports shorter DAPT.
- Use ARC‑HBR to guide DAPT duration, choice of P2Y12, and adjuncts like PPI therapy.
- Document the rationale when deviating from standard durations based on HBR status.
- Aspirin monotherapy is standard after completion of DAPT in many patients (eg 6–12 months as indicated).
- In HBR or very high bleeding risk, consider early transition to single antiplatelet therapy (SAPT) — often clopidogrel or aspirin depending on strategy.
- If P2Y12 monotherapy chosen (eg ticagrelor), aspirin may be stopped early after initial DAPT period.
- Long‑term aspirin indicated for most unless contraindications or patient preference favors P2Y12 monotherapy.
- Decisions should weigh ischemic protection vs bleeding and involve shared decision‑making.
- Assess urgency: if surgery can be delayed, complete recommended DAPT duration when feasible.
- If surgery unavoidable, balance bleeding vs thrombosis risk — consult surgeon and cardiology.
- For high bleeding procedures, consider stopping P2Y12 (timing: clopidogrel 5 days, prasugrel 7 days, ticagrelor 5 days) with aspirin often continued if safe.
- If very high thrombosis risk (recent DES ≤1 month or complex PCI), consider bridging strategy and multidisciplinary discussion.
- Document plan, and resume P2Y12 as soon as surgical bleeding risk allows.
- Clopidogrel efficacy reduced in CYP2C19 loss‑of‑function carriers due to impaired activation.
- Ticagrelor and prasugrel do not require CYP2C19 activation and are preferred in such patients.
- Genotype testing can guide therapy but is not universally required in all settings.
- Consider ticagrelor/prasugrel especially in ACS or high ischemic risk when genotype suggests poor clopidogrel response.
- Balance bleeding risk and cost/availability when switching agents based on genotype.
- Prasugrel is contraindicated in patients with prior stroke/TIA due to excess intracranial bleeding risk.
- Ticagrelor or clopidogrel may be used depending on ischemic vs bleeding risk and indication.
- Evaluate cerebrovascular disease severity and consider neurology consultation if unclear.
- When extending DAPT for ischemic protection, weigh the elevated intracranial bleed risk carefully.
- Document rationale and favor agents with safer cerebrovascular profiles when necessary.
- Assess severity and hemodynamic stability; resuscitate and localize bleeding source promptly.
- Start supportive care (IV fluids, blood products) as indicated and reverse anticoagulants if present per guidance.
- Consider holding P2Y12 agent temporarily; continue aspirin in many cases unless major bleed.
- Use endoscopic, radiologic, or surgical interventions to control bleeding where appropriate; start PPI for GI bleeds.
- After stabilization, reassess need for DAPT duration, possible agent change, and involve multidisciplinary team.
- Complex PCI (eg ≥3 stents, bifurcation with 2 stents, long total stent length, CTO, left main) confers higher ischemic risk.
- Standard approach: 12 months DAPT for ACS or at least 6–12 months for elective depending on bleeding risk.
- Consider longer DAPT (>12 months) for select patients with low bleeding risk and high ischemic risk.
- Ensure optimal stent technique, intravascular imaging, and contemporary DES selection to minimize thrombosis risk.
- Discuss prolonged therapy risks/benefits with patient and document decision-making.
- Routine platelet function testing is not universally recommended for all patients on DAPT.
- Testing may be considered in high‑risk scenarios (recurrent ischemia, stent thrombosis, suspected clopidogrel resistance).
- Genotype testing for CYP2C19 can be useful to identify clopidogrel non‑responders.
- If testing shows high on‑treatment platelet reactivity, consider switching to ticagrelor/prasugrel if not contraindicated.
- Interpret results in clinical context — testing doesn’t replace clinical judgment.
- CKD increases both ischemic and bleeding risks; individualize DAPT duration carefully.
- Ticagrelor is generally usable across CKD stages; prasugrel and clopidogrel decisions depend on stage and comorbidities.
- Prefer shorter durations in patients with advanced CKD and high bleeding tendency.
- Monitor hemoglobin, renal function, and drug interactions closely; adjust doses of concomitant medications as needed.
- Coordinate with nephrology for patients on dialysis or with rapidly changing renal function.
- Start PPI therapy in patients at risk of GI bleeding (history of ulcer, older age, concomitant NSAID use).
- Optimize blood pressure control and avoid unnecessary anticoagulants or interacting drugs.
- Use radial access for PCI to reduce access‑site bleeding risk when feasible.
- Correct modifiable bleeding risks (treat anemia, manage CKD, review concomitant antithrombotic therapy).
- Educate patients on bleeding signs and ensure regular follow‑up for early detection.
- P2Y12 monotherapy (eg ticagrelor or clopidogrel) can follow very short DAPT in selected patients to reduce bleeding.
- TWILIGHT and other trials support ticagrelor monotherapy after 3 months of DAPT in high‑risk patients.
- Consider P2Y12 monotherapy for patients with HBR where aspirin discontinuation reduces bleeding without increasing ischemic events.
- Choice of P2Y12 agent should be based on prior tolerance and ischemic risk.
- Ensure clear documentation and follow‑up when deviating from standard aspirin‑based SAPT.
- Poor stent deployment, underexpansion, malapposition, and incomplete lesion coverage increase risk.
- Patient factors: diabetes, renal dysfunction, low LVEF, high platelet reactivity.
- Procedural complexity: bifurcation 2‑stent techniques, long stent length, small vessel diameter.
- Premature discontinuation of DAPT is a major modifiable risk factor for stent thrombosis.
- Use intravascular imaging (IVUS/OCT) when needed to optimize stent result and reduce thrombosis risk.
- Advanced age increases bleeding risk; consider shorter DAPT (eg 3–6 months) based on individual risk.
- Adjust prasugrel dosing or avoid prasugrel in patients >75 years (consider 5 mg or alternative).
- Consider ticagrelor with caution for dyspnea and bradyarrhythmia; clopidogrel may be preferred if bleeding risk high.
- Use ARC‑HBR and frailty assessments to guide duration and agent selection.
- Engage in shared decision‑making and document rationale for chosen strategy.
- Left main PCI, particularly with complex bifurcation stenting, carries higher ischemic risk and often warrants at least 12 months DAPT if bleeding risk allows.
- Consider prolonged DAPT in patients with additional ischemic risk factors and good bleeding profile.
- Optimize stent technique (DK crush where appropriate) and use intravascular imaging to minimize restenosis/thrombosis.
- Balance decision with patient comorbidities — in HBR consider shorter DAPT with rigorous follow‑up.
- Multidisciplinary discussion (heart team) recommended for high‑risk anatomies.
- Diabetes increases ischemic risk, including stent thrombosis and recurrent MI, often favoring more potent P2Y12 agents (ticagrelor/prasugrel).
- Standard DAPT durations apply, but clinicians may favor extension in diabetics with low bleeding risk.
- Monitor glycemic control as poor control associates with worse outcomes despite antiplatelet therapy.
- Consider genotype and platelet function if recurrent events occur while on clopidogrel.
- Individualize therapy, balancing bleeding propensity common in diabetics with comorbid CKD.
- Stent thrombosis is a life‑threatening event—admit, revascularize emergently, and optimize antithrombotic therapy.
- Investigate and correct procedural causes (malapposition, underexpansion) with imaging-guided PCI if feasible.
- Use more potent P2Y12 agent (ticagrelor/prasugrel) unless contraindicated and consider longer DAPT duration thereafter.
- Evaluate for adherence, drug interactions, and clopidogrel resistance/genotype if previously on clopidogrel.
- Plan closer follow‑up and secondary prevention optimization (statins, BP control, glycemic control).
- Switch when there is intolerance (eg ticagrelor‑related dyspnea) or contraindication (prasugrel after stroke/TIA).
- Switch from clopidogrel to ticagrelor/prasugrel if high on‑treatment platelet reactivity or recurrent ischemia.
- Loading doses may be required when switching from clopidogrel to ticagrelor/prasugrel—follow protocol for safe transition.
- When de‑escalating (eg ticagrelor → clopidogrel), consider platelet function or genotype guidance to ensure efficacy.
- Document reason for switch and ensure patient education on new dosing and side effects.
- High‑intensity statins reduce recurrent ischemic events and likely lower stent thrombosis risk when used long term.
- Start or continue high‑intensity statin therapy unless contraindicated, aiming for LDL targets per guidelines.
- Statins have plaque stabilizing and anti‑inflammatory effects that complement antiplatelet therapy.
- Monitor liver enzymes and counsel on statin‑related side effects to maintain adherence.
- Coordinate lipid clinic follow‑up for aggressive secondary prevention post‑PCI.
- Bioresorbable scaffolds historically carried higher thrombosis risk and often required longer DAPT (≥12 months, sometimes longer) depending on device and patient factors.
- Device generation and operator experience affect recommended duration—follow device‑specific guidance.
- In HBR patients, balance risk and consider close monitoring if shorter DAPT is necessary.
- Given variable data, consider individualized plan with careful follow‑up and low threshold for imaging if concerns arise.
- Prefer contemporary DES in most cases to avoid prolonged DAPT associated with older scaffolds.
- Provide clear discharge instructions with dosing schedule and duration written explicitly.
- Address cost and access—consider generics or assistance programs if cost is a barrier.
- Use pillboxes, follow‑up calls, and reminders to support adherence.
- Educate patients on the consequences of premature discontinuation (stent thrombosis risk).
- Coordinate with primary care for refill continuity and monitoring of side effects.
- Use PPI co‑therapy for patients at increased risk of GI bleeding (history of ulcer, older age, concomitant NSAIDs or steroids).
- PPI reduces upper GI bleeding risk without significant interaction with clopidogrel in most cases; choose agents with lower CYP2C19 interaction when concerned.
- Do not routinely prescribe PPIs to every DAPT patient—target high‑risk individuals.
- Document indication and reassess ongoing need at follow‑up.
- Coordinate with gastroenterology for recurrent GI bleed cases and eradicate H. pylori when present.
- Platelet count thresholds guide management: for counts <50k, many clinicians avoid potent antiplatelets; for 50–100k use caution with clopidogrel preferred.
- Assess reversible causes of thrombocytopenia and consult hematology for guidance if counts are low.
- Balance thrombosis risk versus bleeding—consider shorter DAPT and choose less potent agents where appropriate.
- Monitor platelet counts and bleeding signs closely and adjust therapy dynamically.
- Document multidisciplinary discussion and informed consent when deviating from standard protocols.
- Low‑dose aspirin (75–100 mg daily) is standard in combination with P2Y12 inhibitors for DAPT.
- Higher aspirin doses increase bleeding without clear additional ischemic benefit in most settings.
- In East Asian populations, lower aspirin doses may be favored due to higher bleeding propensity.
- Adjust dose when needed (eg enteric coated formulations) and consider patient weight and comorbidities.
- Document rationale if deviating from low‑dose standard (eg specific clinical trials or unique patient factors).
- Inform patients about common bleeding signs: melena, hematemesis, hematuria, unusual bruising, prolonged bleeding from cuts.
- Advise immediate medical contact for major bleeding, syncope, chest pain, or sudden neurological symptoms.
- Discuss minor bleed management and when to seek urgent care—provide written instructions and emergency contact.
- Encourage avoidance of OTC NSAIDs and other medications that increase bleeding risk unless approved by clinician.
- Arrange early follow‑up to reassess therapy and reinforce education.
- Yes—many supplements (eg ginkgo, garlic, fish oil in high doses, ginger) can increase bleeding risk.
- Ask explicitly about herbal and OTC supplements at discharge and follow‑up.
- Advise stopping or reviewing supplements with clinician when starting DAPT.
- Document counseling and provide patient‑friendly lists of common agents to avoid.
- Coordinate with pharmacy for potential interactions with prescribed antiplatelet agents.
- Evaluate adherence and drug interactions; confirm the patient is actually taking prescribed agents.
- Assess for stent restenosis or new lesions—perform ischemia testing or angiography as indicated.
- Consider switching to a more potent P2Y12 agent (ticagrelor/prasugrel) if on clopidogrel and no contraindications.
- Perform platelet function or genotype testing if clopidogrel resistance suspected to guide de‑escalation/escalation.
- Optimize other secondary prevention measures (statins, BP, diabetes control) alongside antiplatelet adjustments.
- Early follow‑up within 1–2 weeks to confirm adherence, tolerability, and arrange labs if needed.
- Review bleeding signs and assess need for PPI, adjust other meds, and manage side effects at each visit.
- Plan reassessment at 3, 6, and 12 months to decide on continuation or cessation based on events and risk scores.
- More frequent follow‑up for HBR patients, those on OACs, or those with complicated procedures.
- Ensure primary care and cardiology share responsibility for long‑term medication management.
- Minor procedures with low bleeding risk may proceed without stopping DAPT, but consult proceduralist.
- For high bleeding risk procedures, stop P2Y12 per standard washout intervals (clopidogrel 5 days, ticagrelor 5 days, prasugrel 7 days) if safe.
- Aspirin is often continued for many procedures unless bleeding risk dictates otherwise.
- Coordinate timing to minimize interruption—reschedule elective procedures when possible to complete DAPT period.
- Document plan and resume antiplatelet therapy promptly after procedure when bleeding risk controlled.
- Heart failure and low LVEF increase ischemic risk—consider this when weighing DAPT extension decisions.
- Balance against comorbidities (renal dysfunction, anemia) which may increase bleeding risk.
- Optimize heart failure therapy (ACEi/ARB/ARNI, beta‑blocker, MRA) as part of secondary prevention along with antiplatelets.
- Use DAPT score and clinical judgement to decide on prolonged DAPT in those with severe LV dysfunction.
- Monitor renal function and electrolytes closely when on polypharmacy regimens.
- True IgE‑mediated aspirin allergy is rare; distinguish from intolerance (bronchospasm, GI symptoms).
- If aspirin truly contraindicated, consider P2Y12 monotherapy as alternative SAPT after initial DAPT period.
- Aspirin desensitization may be considered in patients who strongly require aspirin and have manageable reactions, under specialist care.
- Collaborate with allergy/immunology for testing and desensitization protocols if necessary.
- Document allergy details clearly and ensure alternative antiplatelet strategy is communicated to all caretakers.
- Liver disease may increase bleeding risk due to coagulopathy and thrombocytopenia—individualize DAPT decisions accordingly.
- Prefer less potent agents (clopidogrel) where bleeding risk high; involve hepatology when severe dysfunction present.
- Monitor INR, platelets, and liver function tests regularly while on antiplatelets.
- Correct reversible coagulopathy (vitamin K deficiency) before elective procedures if feasible.
- Document risks and engage in shared decision‑making given variability of hepatic impairment effects.
- Explain purpose, exact duration, dosing schedule, and what to do if a dose is missed.
- Describe bleeding symptoms that require urgent attention and medications/supplements to avoid.
- Provide written plan with contact numbers, follow‑up appointments, and prescription info for refills.
- Discuss lifestyle measures (avoid heavy alcohol, report falls) and coordinate with primary care for continuity.
- Emphasize importance of adherence to prevent stent thrombosis and recurrent ischemic events.
- Default DAPT duration: 12 months for ACS, 6 months for elective PCI; shorten for HBR and individualize decisions.
- Choose P2Y12 agent based on ischemic vs bleeding risk, contraindications, and patient factors (genotype, tolerance).
- Use ARC‑HBR and DAPT score to guide duration; reassess at 3, 6, and 12 months as needed.
- Minimize triple therapy duration in patients requiring OAC and favor DOAC + clopidogrel when appropriate.
- Educate patients, optimize secondary prevention (statins, BP, diabetes), and document shared decision‑making.
Post PCI DAPT, Dual antiplatelet therapy after PCI, Duration of DAPT after stenting, DAPT guidelines 2025, Drug-eluting stent DAPT duration, Bare-metal stent DAPT, Aspirin + P2Y12 inhibitor therapy, Ticagrelor after PCI, Prasugrel after PCI, Clopidogrel after PCI, High bleeding risk DAPT, Extended DAPT therapy, Short-course DAPT, ACS vs stable CAD DAPT, DAPT score, PRECISE-DAPT score, Risk of stent thrombosis, Bleeding risk after PCI, DAPT de-escalation strategies, Stopping DAPT early, Optimal duration of DAPT after DES, When to discontinue DAPT after PCI, Ticagrelor vs clopidogrel after MI, DAPT for diabetics after PCI, DAPT in complex PCI, Antiplatelet therapy for left main PCI, DAPT after chronic total occlusion PCI, DAPT for bifurcation stenting, Triple therapy in PCI with AF, Single antiplatelet therapy after DAPT, How long should DAPT be continued after PCI, Recommended antiplatelet therapy after stenting, Shortening DAPT in high bleeding risk, When to use ticagrelor instead of clopidogrel, Patients needing prolonged DAPT, DAPT after balloon angioplasty, Does DAPT reduce stent thrombosis, Early discontinuation of DAPT, Switching antiplatelet agents after PCI, Bleeding complications with DAPT, platelet inhibition, ischemic event prevention, stent thrombosis prevention, thrombotic risk stratification, bleeding risk stratification, antiplatelet pharmacology, PCI complication reduction, ACS management guidelines, cardiology guideline updates, P2Y12 inhibitor comparison, dual antiplatelet therapy guidelines, best antiplatelet therapy after stenting, DAPT evidence trials, ischemia vs bleeding balance, tailoring DAPT duration, antiplatelet therapy post MI







