Cangrelor
CANGRELOR — High-Yield, Exam-Oriented Summary (DM / NEET-SS Level)
Class & Mechanism
- Intravenous, direct P2Y12 receptor antagonist
- Reversible, non-thienopyridine
- Produces immediate platelet inhibition (within minutes)
- Platelet function normalizes ~60 minutes after discontinuation
Pharmacokinetics
- Onset: 2–3 minutes
- Half-life: 3–6 minutes
- Offset: Rapid (no accumulation)
- Metabolism: Plasma dephosphorylation (not hepatic/renal)
- No dose adjustment for renal or hepatic dysfunction
Indications (Guideline-Supported)
- PCI patients who:
- Are P2Y12-naïve, OR
- Cannot take oral agents (intubated, shock, vomiting), OR
- Need rapid on–off platelet inhibition
- Bridging therapy when oral P2Y12 must be held pre-CABG (off-label but evidence-based)
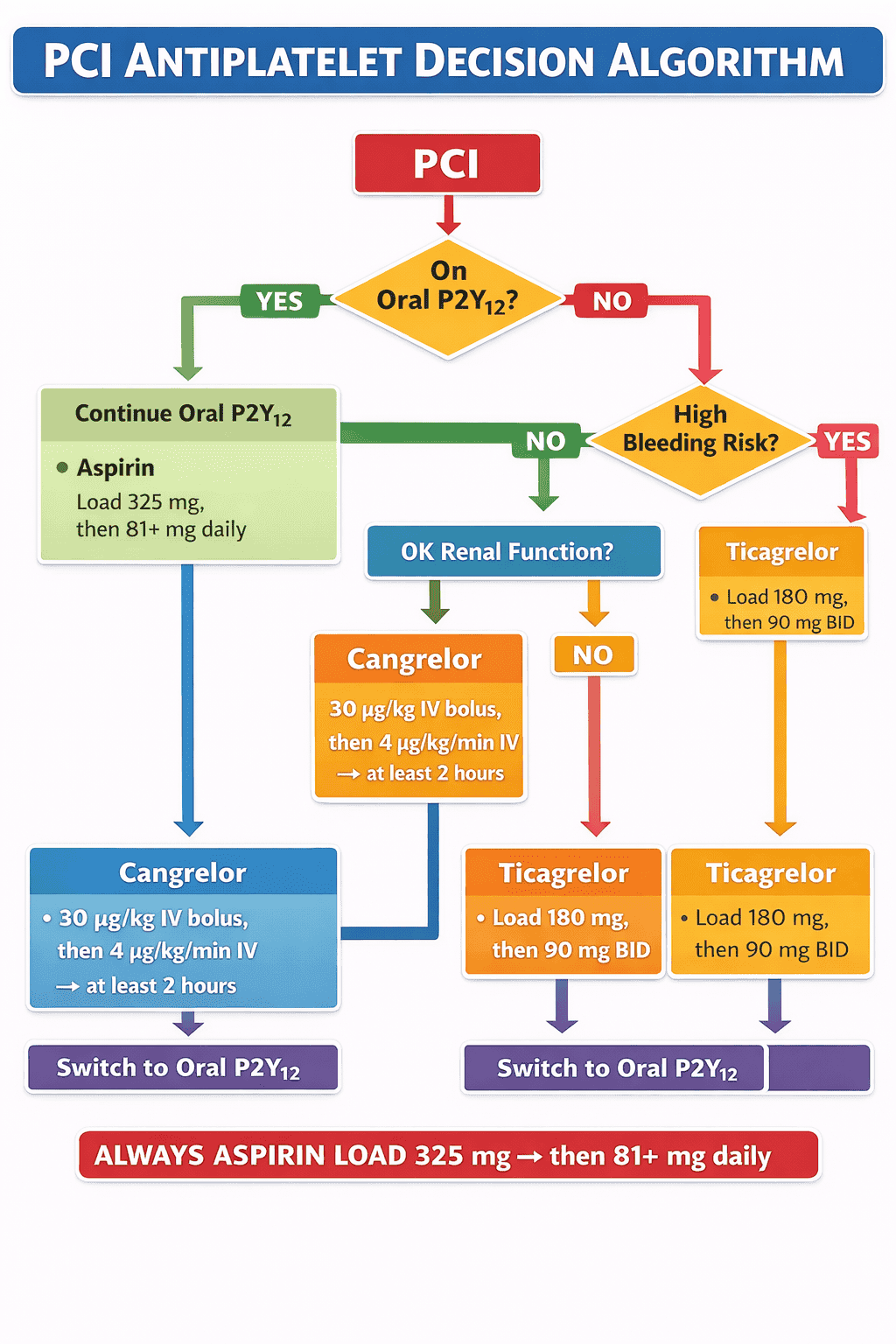
Dose (Must Memorize)
- Bolus: 30 μg/kg IV
- Infusion: 4 μg/kg/min
- Start immediately before PCI → continue at least 2 hours or for duration of PCI
Key Clinical Trials
- CHAMPION PCI
- CHAMPION PLATFORM
- CHAMPION PHOENIX (most important)
- ↓ Periprocedural MI
- ↓ Acute stent thrombosis
- No significant ↑ in severe bleeding (GUSTO severe)
Advantages Over Oral P2Y12
- No need for GI absorption
- Effective in shock / cardiac arrest
- Predictable inhibition (no clopidogrel resistance)
- Rapid reversibility → safer if urgent surgery required
Critical Drug Interactions (Very Exam-Relevant)
- Clopidogrel / Prasugrel
- Must be given AFTER stopping cangrelor
- Ticagrelor
- Can be given during or after infusion
Reason: cangrelor competitively blocks binding of active metabolites of thienopyridines
Bleeding Profile
- ↑ Minor bleeding
- No significant increase in life-threatening bleeding
- Avoid if active pathological bleeding
Special Situations
- STEMI with cardiogenic shock
- Out-of-hospital cardiac arrest PCI
- High thrombus burden
- Complex PCI (LM, bifurcation) when oral loading unreliable
Comparison Snapshot
- Cangrelor = IV, reversible, ultra-fast
- GP IIb/IIIa inhibitors = downstream, higher bleeding
- Oral P2Y12 = delayed, variable absorption
One-Line Exam Pearl
Cangrelor is the only IV P2Y12 inhibitor providing immediate, reversible platelet inhibition during PCI, with rapid offset and proven reduction in acute stent thrombosis.
CANGRELOR — 20 Ultra–High-Difficulty Trial-Based MCQs
1. In CHAMPION PHOENIX, the reduction in the primary composite endpoint with cangrelor was driven predominantly by:
A. Reduction in all-cause mortality
B. Reduction in periprocedural MI and acute stent thrombosis
C. Reduction in major bleeding
D. Reduction in stroke
CHAMPION PHOENIX showed benefit mainly from fewer periprocedural MIs and acute stent thrombosis, not mortality.
2. Why must clopidogrel be administered only after stopping cangrelor infusion?
A. Increased bleeding risk
B. Competitive inhibition of P2Y12 receptor by cangrelor
C. Delayed hepatic activation
D. CYP3A4 interaction
Cangrelor blocks receptor binding of clopidogrel’s active metabolite, nullifying its effect if given concurrently.
3. Which oral P2Y12 inhibitor can be safely loaded during cangrelor infusion?
A. Clopidogrel
B. Prasugrel
C. Ticagrelor
D. None
Ticagrelor binds a different receptor site and is not blocked by cangrelor.
4. The very short half-life of cangrelor is primarily due to:
A. Rapid plasma dephosphorylation
B. Renal clearance
C. Hepatic metabolism
D. Platelet uptake
Cangrelor is metabolized by plasma ectonucleotidases, independent of liver or kidney function.
5. In which scenario is cangrelor most strongly supported by evidence?
A. Chronic stable angina on medical therapy
B. P2Y12-naïve patient undergoing ad-hoc PCI
C. Post-CABG secondary prevention
D. Long-term DAPT maintenance
Cangrelor is indicated during PCI when rapid platelet inhibition is required and oral loading is unreliable.
6. Compared with GP IIb/IIIa inhibitors, cangrelor offers which key advantage?
A. Stronger platelet inhibition
B. Lower severe bleeding with rapid reversibility
C. Oral bioavailability
D. Longer platelet inhibition
GP IIb/IIIa inhibitors are downstream and associated with higher bleeding risk.
7. The standard bolus dose of cangrelor during PCI is:
A. 10 μg/kg
B. 30 μg/kg
C. 60 μg/kg
D. Weight-independent fixed dose
Dose is 30 μg/kg bolus followed by 4 μg/kg/min infusion.
8. Platelet function returns to near normal approximately how long after stopping cangrelor?
A. 10 minutes
B. 60 minutes
C. 6 hours
D. 24 hours
Rapid offset is a defining feature, enabling urgent surgery if required.
9. Which bleeding definition showed no significant increase with cangrelor in CHAMPION PHOENIX?
A. TIMI minor
B. ACUITY
C. GUSTO severe
D. BARC 2–5
Severe/life-threatening bleeding was not increased.
10. Which patient profile derives maximum pharmacodynamic benefit from cangrelor?
A. Elective PCI with prior ticagrelor
B. STEMI with cardiogenic shock and vomiting
C. Chronic kidney disease stage 5
D. Stable angina awaiting CTCA
Oral P2Y12 absorption is unreliable in shock; IV cangrelor bypasses this.