Brockenbrough–Braunwald–Morrow Sign: MCQs
Q1. The Brockenbrough–Braunwald–Morrow sign is typically observed in:
A. Aortic stenosis
B. Hypertrophic obstructive cardiomyopathy
C. Mitral regurgitation
D. Pulmonary stenosis
It is a hemodynamic sign seen in hypertrophic obstructive cardiomyopathy during catheterization.
Q2. The mechanism of the sign involves:
A. Increased preload causing enhanced stroke volume
B. Decreased afterload leading to better ejection
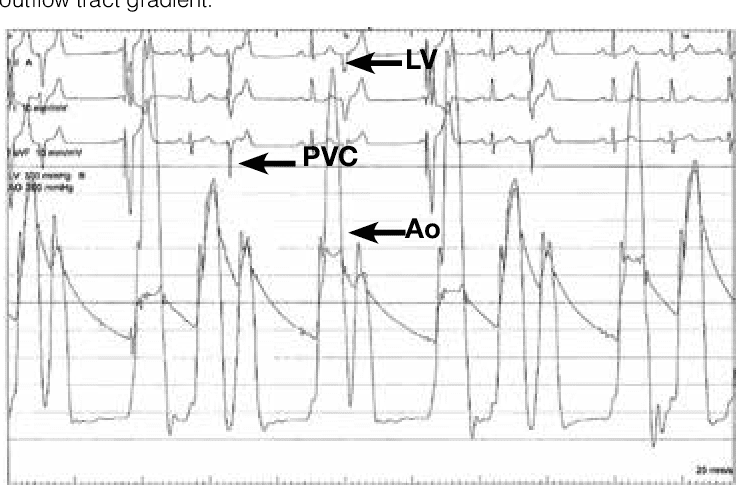
C. Post-extrasystolic potentiation with paradoxical fall in pulse pressure
D. Bradycardia-induced augmentation of filling
After a PVC, contractility increases, but in HOCM, obstruction worsens, so arterial pulse pressure falls instead of rising.
Q3. In which procedure is the Brockenbrough sign typically elicited?
A. Cardiac catheterization
B. Echocardiography
C. MRI
D. CT angiography
It is classically demonstrated during cardiac catheterization after inducing a premature beat.
Q4. What happens to the left ventricular systolic pressure after a PVC in HOCM?
A. Falls significantly
B. Remains unchanged
C. Normal post-extrasystolic potentiation
D. Rises markedly
Post-extrasystolic potentiation increases LV systolic pressure, but paradoxically the arterial pulse pressure drops in HOCM.
Q5. The paradoxical response in the Brockenbrough sign helps differentiate HOCM from:
A. Aortic stenosis
B. Mitral valve prolapse
C. Tricuspid regurgitation
D. Pulmonary hypertension
In aortic stenosis, the arterial pulse pressure increases after PVC, unlike the paradoxical fall in HOCM.
Q6. Which artery pressure tracing shows the paradoxical fall?
A. Left atrial
B. Left ventricular
C. Aortic
D. Pulmonary artery
The paradoxical fall is noted in the aortic pressure tracing despite increased LV systolic pressure.
Q7. What causes worsening obstruction after PVC in HOCM?
A. Reduced preload
B. Increased contractility with systolic anterior motion of mitral valve
C. Vasodilation
D. Slower heart rate
Post-PVC, the increased contractility accentuates dynamic LVOT obstruction via SAM of the mitral valve.
Q8. Which clinical scenario demonstrates the Brockenbrough sign most clearly?
A. Acute myocardial infarction
B. Chronic hypertension
C. Mitral stenosis
D. Hypertrophic obstructive cardiomyopathy with catheterization
It is specific for HOCM when elicited during invasive hemodynamic study.
Q9. Which of the following does NOT show the Brockenbrough sign?
A. Fixed subaortic stenosis
B. Hypertrophic obstructive cardiomyopathy
C. Dynamic LVOT obstruction
D. Idiopathic hypertrophic subaortic stenosis
Fixed subaortic obstruction behaves like valvular AS, so it does not demonstrate the paradoxical fall.
Q10. The Brockenbrough sign is helpful in:
A. Assessing mitral regurgitation severity
B. Detecting pulmonary hypertension
C. Differentiating dynamic vs fixed LVOT obstruction
D. Evaluating right heart pressures
It helps distinguish dynamic obstruction in HOCM from fixed obstruction like AS.
Q11. Who first described the Brockenbrough sign?
A. Braunwald alone
B. Morrow alone
C. Wiggers
D. Brockenbrough, Braunwald, and Morrow
The sign is named after Brockenbrough, Braunwald, and Morrow who described it in HOCM.
Q12. In normal hearts, what happens to aortic pulse pressure after a PVC?
A. Falls
B. Rises
C. No change
D. Becomes irregular
Normally, post-extrasystolic potentiation increases stroke volume and aortic pulse pressure.
Q13. The sign is useful in confirming:
A. Mitral stenosis
B. Dilated cardiomyopathy
C. Dynamic LVOT obstruction
D. Pulmonary embolism
The paradoxical response confirms the presence of dynamic LVOT obstruction in HOCM.
Q14. Which hemodynamic parameter rises post-PVC in HOCM?
A. LV systolic pressure
B. Aortic pulse pressure
C. Mean arterial pressure
D. Right atrial pressure
The LV systolic pressure rises post-PVC due to potentiation, but the aortic pulse pressure falls.
Q15. The paradoxical pulse pressure fall is due to:
A. Bradycardia
B. Increased venous return
C. Decreased contractility
D. Worsened LVOT obstruction
Increased contractility post-PVC worsens the obstruction, reducing forward flow into the aorta.
Q16. The Brockenbrough sign is absent in:
A. HOCM
B. Valvular aortic stenosis
C. Dynamic subaortic obstruction
D. IHSS
In valvular AS, the expected response post-PVC is increased aortic pulse pressure, not a fall.
Q17. What type of murmur is associated with the Brockenbrough sign condition?
A. Mid-diastolic murmur
B. Early diastolic murmur
C. Harsh systolic ejection murmur at left sternal border
D. Continuous murmur
HOCM produces a harsh systolic ejection murmur best heard at the left sternal border.
Q18. The sign provides insight into which pathophysiologic mechanism?
A. Dynamic LVOT obstruction
B. Pulmonary hypertension
C. Right-to-left shunting
D. Aortic regurgitation
It highlights the dynamic nature of LVOT obstruction in HOCM.
Q19. Which therapy reduces the occurrence of the Brockenbrough sign?
A. Diuretics
B. Inotropes
C. Vasodilators
D. Negative inotropes like beta-blockers
Beta-blockers reduce contractility, alleviating dynamic LVOT obstruction and thus the sign.
Q20. The Brockenbrough sign confirms the diagnosis when combined with:
A. Coronary angiography
B. Pressure tracings showing LV–aortic gradient post-PVC
C. Echocardiographic Doppler of mitral inflow
D. Right heart catheterization
The hallmark is increased LV systolic pressure but decreased aortic pulse pressure post-PVC, confirming dynamic obstruction.
Published in Methodist DeBakey Cardiovascular Journal 2014 – Alejandro TrevinoJ. Buergler