WPW Syndrome
WPW Syndrome
Causes
- Accessory pathway: In a healthy heart, electrical signals travel along a specific route to regulate the heartbeat. In WPW syndrome, an extra or “accessory” pathway (often called the bundle of Kent) allows electrical signals to bypass the normal path, causing the ventricles to activate prematurely. This can trigger a very rapid, abnormal heartbeat called supraventricular tachycardia (SVT).
- Genetic link: While the cause is often unknown, a small number of familial cases have been linked to a gene mutation.
- Associated conditions: WPW syndrome has been associated with other heart conditions, such as Ebstein anomaly.
Symptoms
WPW syndrome symptoms appear when a fast heartbeat occurs and vary in frequency and severity among individuals. Some people with the accessory pathway never experience symptoms and do not have WPW syndrome, but a condition known as “WPW pattern”.
Symptoms may include:
- A rapid, fluttering, or pounding heartbeat (palpitations)
- Dizziness or lightheadedness
- Fainting (syncope)
- Shortness of breath
- Chest pain or tightness
- Anxiety
- Fatigue
Diagnosis
WPW syndrome is often diagnosed using an electrocardiogram (ECG), which measures the heart’s electrical activity. During an episode of tachycardia, an ECG will show a heart rate faster than 100 beats per minute. Distinctive ECG findings for WPW include:
- A short PR interval
- A “delta wave,” a slurred, initial upstroke on the QRS complex
- A wide QRS complex
WPW Syndrome-The classic triad of electrocardiographic findings :
WPW Syndrome
short PR interval, broad QRS complex and delta wave.
Other diagnostic tests may include:
- Holter monitor: A wearable device that records the heart’s electrical activity over 24 hours or longer.
- Electrophysiological (EP) study: An invasive procedure to map the heart’s electrical system and pinpoint the location of the extra pathway.
Treatment and outlook
Treatment for WPW is based on whether the person has symptoms and how serious they are.
- For asymptomatic individuals: Those with the WPW pattern but no symptoms usually don’t require treatment.
- For symptomatic individuals: The most common and highly effective treatment is catheter ablation.
- Catheter ablation: A minimally invasive procedure where a doctor uses a catheter to deliver radiofrequency energy to destroy the accessory pathway, curing the condition for most people.
- Medications: Antiarrhythmic drugs can be used to control episodes of rapid heart rate.
- Emergency treatment: In unstable cases, electrical cardioversion can restore a normal heart rhythm.
With appropriate treatment, WPW syndrome can often be cured, and people can lead a normal life. However, left untreated, particularly when paired with other arrhythmias like atrial fibrillation, it can carry a rare but serious risk of sudden cardiac death.
Wolff–Parkinson–White (WPW) Syndrome – Overview
Definition:
WPW syndrome is a pre-excitation disorder of the heart caused by an accessory atrioventricular conduction pathway (bundle of Kent) that allows electrical impulses to bypass the AV node, leading to tachyarrhythmias.
🔹 Key Features
- Pathophysiology
- Accessory pathway directly connects atria to ventricles.
- Conduction bypasses AV nodal delay → early ventricular depolarization.
- May cause re-entrant tachycardias (orthodromic or antidromic).
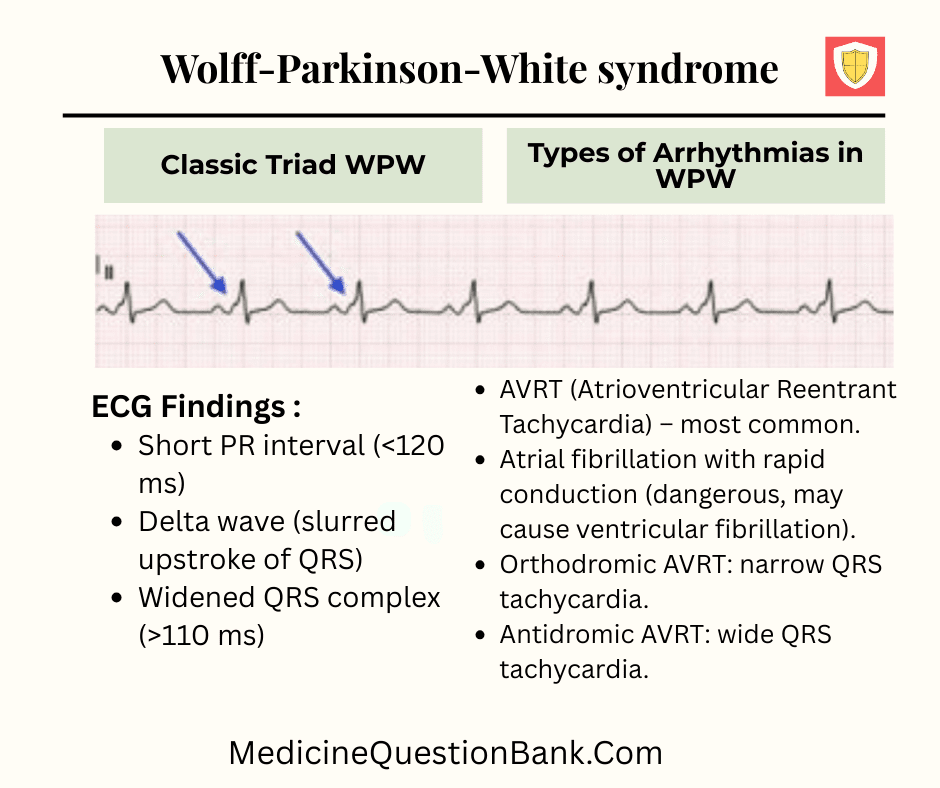
- ECG Findings (Classic Triad):
- Short PR interval (<120 ms)
- Delta wave (slurred upstroke of QRS)
- Widened QRS complex (>110 ms)
- Types of Arrhythmias in WPW:
- AVRT (Atrioventricular Reentrant Tachycardia) – most common.
- Atrial fibrillation with rapid conduction (dangerous, may cause ventricular fibrillation).
- Orthodromic AVRT: narrow QRS tachycardia.
- Antidromic AVRT: wide QRS tachycardia.
- Clinical Presentation:
- Palpitations, dizziness, syncope.
- May be asymptomatic (incidental finding).
- Rarely sudden cardiac death (due to AF → VF).
🔹 Diagnosis
- ECG is diagnostic.
- Electrophysiological study (EPS): confirms pathway location.
- Holter monitoring may detect intermittent pre-excitation.
🔹 Management
- Acute Tachyarrhythmia (Stable):
- Orthodromic AVRT (narrow QRS): Vagal maneuvers → Adenosine → β-blockers/CCBs (avoid if WPW + AF).
- Antidromic AVRT (wide QRS): Procainamide or cardioversion if unstable.
- WPW + Atrial Fibrillation: Avoid AV nodal blockers (adenosine, verapamil, diltiazem, digoxin). Use procainamide or ibutilide.
- Definitive Therapy:
- Catheter ablation of accessory pathway (first-line in symptomatic WPW).
- Asymptomatic WPW:
- Observation or risk stratification with EPS.
- Ablation if high-risk pathway (short refractory period).
🔹 Prognosis
- Good with successful ablation (curative in >95%).
- Risk of sudden death is low but higher in patients with atrial fibrillation and rapid conduction.
| Feature | Details |
|---|---|
| Cause | Accessory pathway (Bundle of Kent) connecting atria and ventricles |
| ECG Triad |
• Short PR interval (<120 ms) • Delta wave (slurred upstroke) • Wide QRS complex (>110 ms) |
| Common Arrhythmias |
• Orthodromic AVRT (narrow QRS) • Antidromic AVRT (wide QRS) • Atrial fibrillation (dangerous) • Atrial flutter |
| Danger | AF can rapidly conduct via accessory pathway → risk of ventricular fibrillation (sudden death) |
| Drugs to Avoid |
• AV nodal blockers (Verapamil, Diltiazem, Digoxin, Adenosine) • These worsen conduction via accessory pathway |
| Drugs of Choice (Acute) |
• Procainamide • Ibutilide • Cardioversion if unstable |
| Definitive Therapy | Radiofrequency catheter ablation (success >95%) |
| Asymptomatic WPW | Observation or risk stratification (EPS) unless high-risk pathway is present |
| Feature | Wolff–Parkinson–White (WPW) Syndrome | Lown–Ganong–Levine (LGL) Syndrome |
|---|---|---|
| Accessory Pathway | Bundle of Kent (direct atrium-to-ventricle conduction) | Bundle of James (atrium-to-His bundle bypassing AV node) |
| PR Interval | Short (<120 ms) | Short (<120 ms) |
| QRS Complex | Wide (>110 ms) due to early ventricular activation | Normal (narrow) |
| Delta Wave | Present (slurred upstroke of QRS) | Absent |
| Mechanism | Direct pre-excitation of ventricles | Bypasses AV nodal delay but still activates ventricles via normal conduction system |
| Typical Arrhythmias | • AVRT (orthodromic & antidromic) • AF with rapid conduction (dangerous) • Atrial flutter | • Paroxysmal supraventricular tachycardia (PSVT) • AV nodal reentrant tachycardia (AVNRT)-like |
| Risk of Sudden Death | Present (AF → VF) | Minimal to none |
| Definitive Treatment | Radiofrequency ablation of accessory pathway | Medical therapy (rarely requires ablation) |
key differences:
WPW: Short PR + Wide QRS + Delta wave.
LGL: Short PR + Normal QRS + No delta wave.
Wolff–Parkinson–White syndrome, WPW syndrome, WPW pattern, Accessory pathway, Bundle of Kent, Pre-excitation syndrome, Short PR interval, Delta wave, Wide QRS complex, Type A WPW, Type B WPW, Type C WPW, Left-sided WPW, Right-sided WPW, Septal WPW, LBBB mimic, RBBB mimic, AV reentrant tachycardia, Orthodromic AVRT, Antidromic AVRT, Pre-excited atrial fibrillation, Supraventricular tachycardia, Ventricular fibrillation, Sudden cardiac death, Procainamide, Ibutilide, Avoid AV nodal blockers, Verapamil contraindication, Digoxin contraindication, Adenosine contraindication, Radiofrequency ablation, Catheter ablation, Electrophysiology study, Lown–Ganong–Levine syndrome, AV nodal reentrant tachycardia, Bundle branch block mimic, Paroxysmal supraventricular tachycardia







