Which of the following statement is true for diagnosis of ventilator associated pneumonia:
[A] Specificity of chest X-ray is very high for its diagnosis [B] Quantitative culture of secretions is required [C] Causative organisms are most frequently found in blood cultures [D] Clinical criteria are sufficient for the diagnosis
ANSWER
[B] Quantitative culture of secretions is required
Clinical criteria for Ventilator-Associated Pneumonia (VAP) are generally not considered sufficient for a definitive diagnosis on their own. While they are essential for initiating early, empirical antibiotic therapy—as waiting for microbiology results can increase mortality—they lack the specificity needed to confirm the infection.
Key Aspects of VAP Diagnosis
Limitations of Clinical Criteria: Symptoms like fever, leukocytosis, and purulent secretions are common in ventilated patients but are not specific to pneumonia. They can be caused by other conditions such as atelectasis, ARDS, or pulmonary embolism.
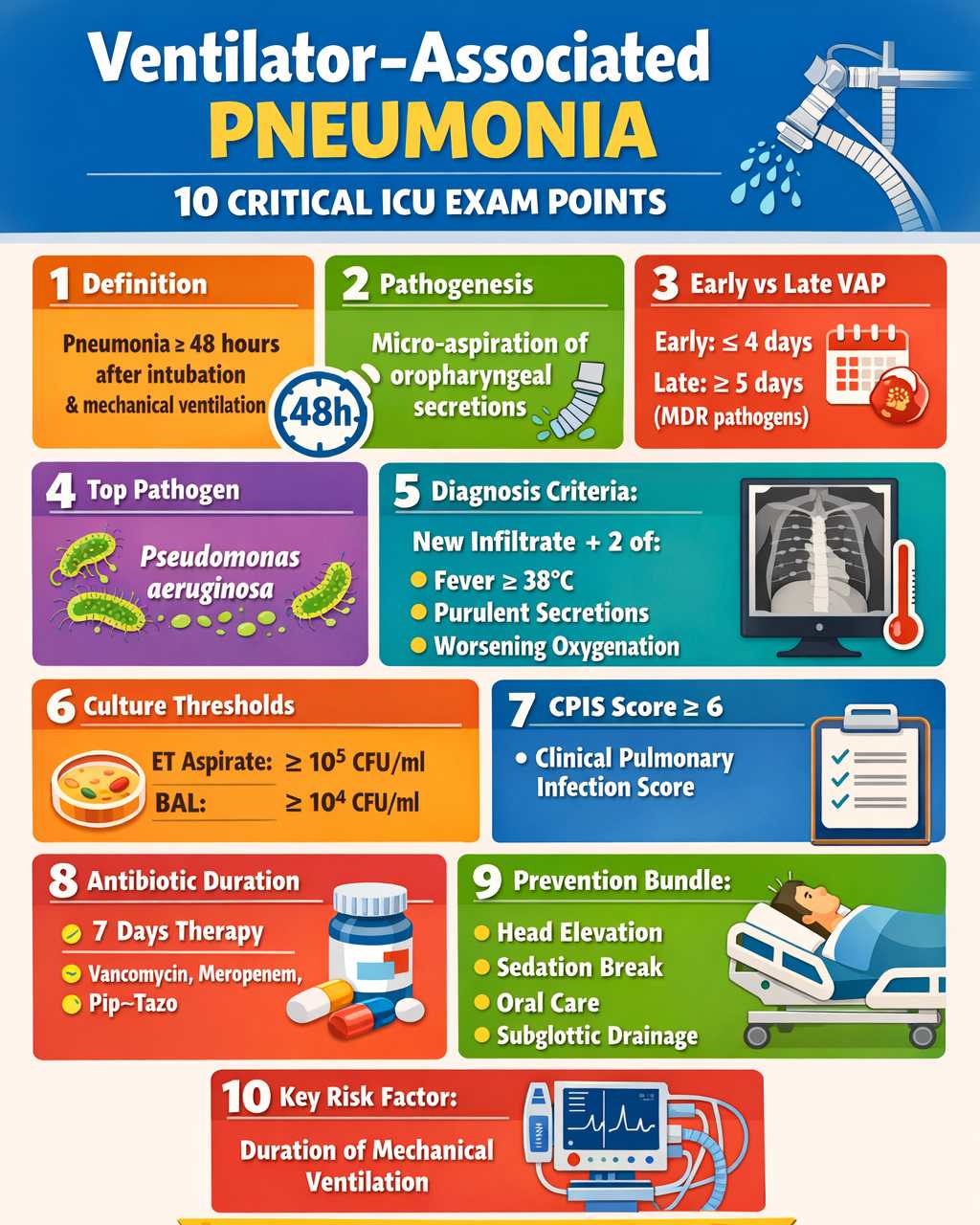
Ventilator-Associated Pneumonia (VAP) is a subtype of Hospital‑Acquired Pneumonia that develops ≥48 hours after endotracheal intubation and initiation of mechanical ventilation. It is one of the most frequent ICU-acquired infections and is associated with increased mortality, prolonged ICU stay, and higher healthcare costs.
1. Definition
Ventilator-Associated Pneumonia (VAP): Pneumonia occurring 48 hours or more after endotracheal intubation, characterized by new lung infiltrates plus clinical evidence of infection.
Related entity: Ventilator‑Associated Pneumonia
Diagnostic suspicion requires:
New/progressive radiographic infiltrate
At least two of the following:
Fever >38 °C
Leukocytosis or leukopenia
Purulent tracheal secretions
Worsening oxygenation
2. Pathogenesis
The principal mechanism is micro-aspiration of colonized secretions from the oropharynx or stomach into the lower respiratory tract.
Key steps
Oropharyngeal colonization
Biofilm formation on endotracheal tube
Micro-aspiration around cuff
Impaired host defense
Risk factors include:
Mechanical ventilation >48 hours
Supine position
Reintubation
Sedation/paralysis
Nasogastric tubes
Prior antibiotics
3. Classification
Early-Onset VAP
Occurs within 4 days of ventilation
Common organisms:
Streptococcus pneumoniae
Haemophilus influenzae
Staphylococcus aureus (MSSA)
Usually antibiotic-sensitive pathogens
Late-Onset VAP
Occurs ≥5 days after ventilation
Often caused by multidrug-resistant organisms (MDROs)
Common organisms:
Pseudomonas aeruginosa
Acinetobacter baumannii
Klebsiella pneumoniae
Methicillin‑resistant Staphylococcus aureus
4. Diagnosis
Clinical criteria
Fever
Leukocytosis
Purulent secretions
Worsening oxygenation
Radiology
Chest X-ray:
New infiltrate
Consolidation
Air bronchograms
Microbiologic diagnosis
Non-invasive
Endotracheal aspirate
Invasive
Bronchoalveolar lavage (BAL)
Protected specimen brush
Quantitative culture thresholds:
Method
Diagnostic count
Endotracheal aspirate
≥10⁵ CFU/ml
BAL
≥10⁴ CFU/ml
Protected brush
≥10³ CFU/ml
5. Clinical Pulmonary Infection Score (CPIS)
Parameters:
Temperature
Leukocyte count
Tracheal secretions
Oxygenation (PaO₂/FiO₂)
Chest X-ray
Culture results
CPIS ≥6 → suggests VAP
6. Treatment
Empiric antibiotics
Depends on early vs late VAP and MDR risk.
Early VAP (no MDR risk)
Ceftriaxone
Ampicillin/sulbactam
Levofloxacin
Late VAP / MDR risk
Broad-spectrum coverage:
Antipseudomonal β-lactam
Piperacillin–tazobactam
Cefepime
Meropenem
PLUS
MRSA coverage
Vancomycin
Linezolid
Duration:
7 days if adequate response
7. Prevention (Ventilator Bundle)
Evidence-based ICU measures:
Head elevation 30–45°
Daily sedation interruption
Daily spontaneous breathing trial
Peptic ulcer prophylaxis
DVT prophylaxis
Oral care with chlorhexidine
Subglottic secretion drainage
These strategies significantly reduce **Ventilator‑Associated Pneumonia incidence.
8. Prognosis
Mortality: 20–50%
Higher in:
MDR infections
septic shock
delayed antibiotics
9. High-Yield Exam Pearls (NEET-SS / ICU)
VAP occurs ≥48 hours after intubation
Most common pathogen:Pseudomonas aeruginosa
CPIS ≥6 suggests VAP
Head elevation 30–45° is the most effective preventive ICU measure
Biofilm on endotracheal tube is a major infection source
Duration of therapy = 7 days in most cases
1. Ventilator-associated pneumonia is defined as pneumonia occurring:
A. Within 24 hours of intubation
B. ≥48 hours after mechanical ventilation
C. ≥24 hours after hospital admission
D. ≥72 hours after ICU admission
VAP is defined as pneumonia developing ≥48 hours after endotracheal intubation.
2. Most common pathogen causing late-onset VAP in ICUs worldwide:
A. Pseudomonas aeruginosa
B. Streptococcus pneumoniae
C. Legionella pneumophila
D. Mycoplasma pneumoniae
Pseudomonas aeruginosa is the leading cause of late-onset ventilator-associated pneumonia.
3. The most important pathophysiologic mechanism in VAP:
A. Micro-aspiration of colonized oropharyngeal secretions
B. Hematogenous spread
C. Lymphatic dissemination
D. Transpleural infection
Microaspiration of colonized secretions around the endotracheal tube cuff is the main mechanism.
4. Diagnostic threshold for BAL culture in suspected VAP:
A. 10² CFU/ml
B. 10³ CFU/ml
C. 10⁴ CFU/ml
D. 10⁵ CFU/ml
BAL quantitative culture ≥10⁴ CFU/ml supports diagnosis of VAP.
5. Diagnostic threshold for protected specimen brush culture:
A. 10⁵ CFU/ml
B. 10³ CFU/ml
C. 10⁴ CFU/ml
D. 10² CFU/ml
Protected specimen brush threshold = ≥10³ CFU/ml.
6. Component NOT included in CPIS score:
A. Temperature
B. Leukocyte count
C. Serum procalcitonin
D. PaO₂/FiO₂ ratio
CPIS includes temp, WBC, oxygenation, secretions, CXR, and cultures—not procalcitonin.
7. Most effective preventive measure for VAP:
A. Head-of-bed elevation 30–45°
B. Routine antibiotic prophylaxis
C. Daily bronchoscopy
D. Continuous sedation
Head-of-bed elevation reduces aspiration and significantly lowers VAP incidence.
8. Early-onset VAP usually occurs:
A. Within first 4 days of ventilation
B. After 7 days
C. After 10 days
D. Only after ICU stay of 1 week
Early VAP = ≤4 days after ventilation.
9. Early-onset VAP most commonly involves:
A. Antibiotic-sensitive organisms
B. Carbapenem-resistant bacteria
C. Multidrug-resistant organisms
D. Fungal pathogens
Early VAP is usually caused by antibiotic-sensitive community organisms.
10. Biofilm formation in VAP occurs primarily on:
A. Endotracheal tube
B. Nasogastric tube
C. Ventilator circuit tubing
D. Central venous catheter
Biofilm formation on the endotracheal tube is a key source of persistent infection.
11. The most common multidrug-resistant pathogen causing VAP in Asian ICUs:
A. Streptococcus pneumoniae
B. Acinetobacter baumannii
C. Moraxella catarrhalis
D. Mycoplasma pneumoniae
Acinetobacter baumannii is a major MDR pathogen in VAP in many Asian ICUs.