Upstream Therapy for Atrial Fibrillation
Upstream Therapy for Atrial Fibrillation (AF)
Definition
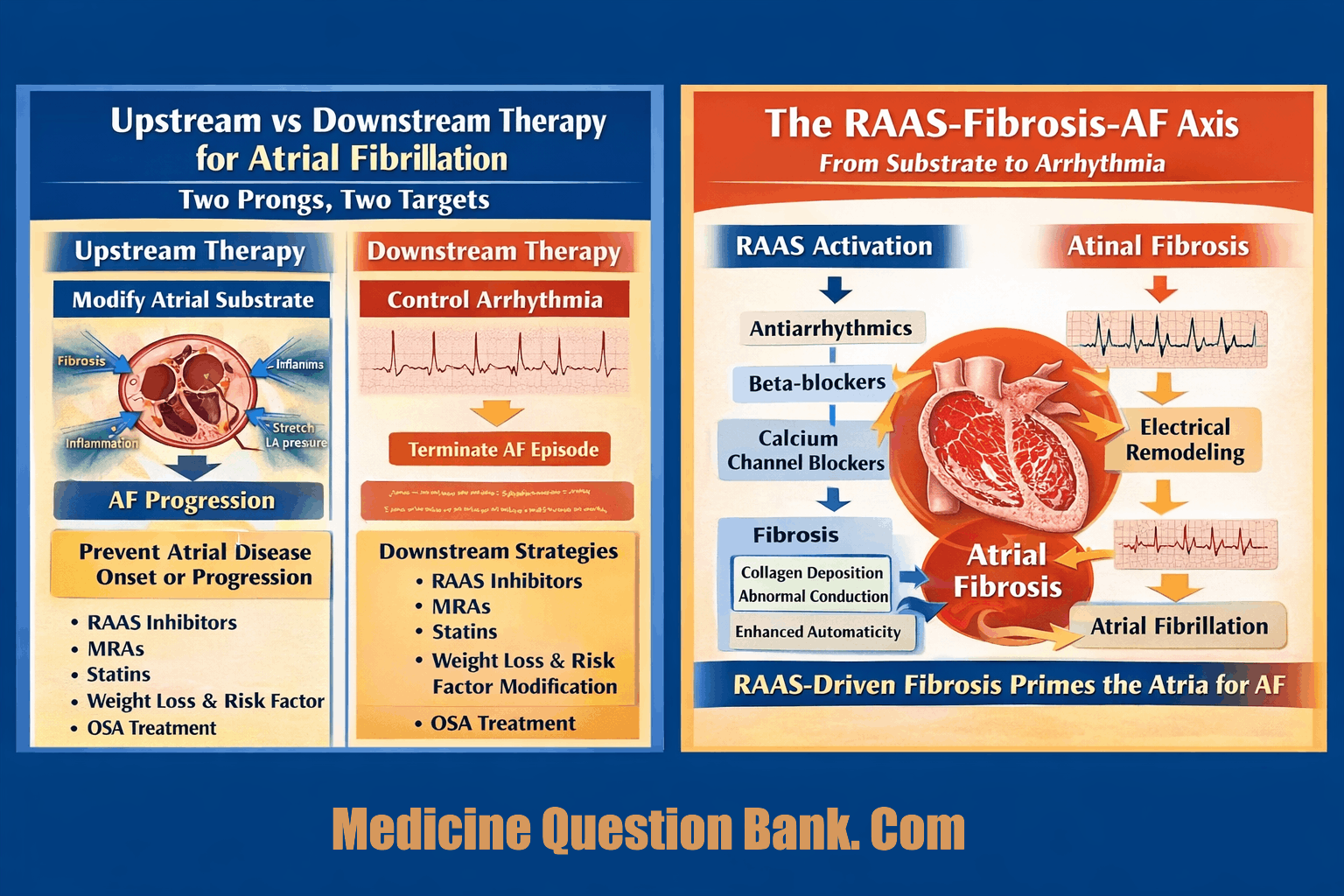
Upstream therapy in atrial fibrillation refers to the use of non–antiarrhythmic, non–rate-control drugs that modify the atrial substrate, thereby preventing AF onset, progression, or recurrence by targeting structural, electrical, and inflammatory remodeling.
It is disease-modifying, not rhythm-terminating.
Rationale
AF is sustained by:
- Atrial fibrosis
- Inflammation
- Oxidative stress
- Neurohormonal activation
- Structural remodeling
Upstream therapies act before AF becomes self-perpetuating (“AF begets AF”).
Major Classes of Upstream Therapies
1. Renin–Angiotensin–Aldosterone System (RAAS) Inhibitors
ACE inhibitors / ARBs / MRAs
Mechanisms
- Reduce atrial fibrosis
- Inhibit TGF-β–mediated collagen deposition
- Decrease atrial stretch and pressure
- Improve electrical homogeneity
Evidence
- Primary prevention of AF in:
- Hypertension
- Heart failure
- LV hypertrophy
- Less effective for secondary prevention in established AF
Key Trials
- LIFE (losartan ↓ new-onset AF)
- CHARM
- Val-HeFT
✅ Most effective upstream therapy
2. Mineralocorticoid Receptor Antagonists (MRAs)
Spironolactone, Eplerenone
Mechanisms
- Potent anti-fibrotic effect
- Reduce atrial remodeling
- Improve diastolic function
Evidence
- Reduced AF burden in HF
- Better atrial reverse remodeling
3. Statins
Mechanisms
- Anti-inflammatory
- Antioxidant
- Improve endothelial function
Evidence
- Strongest benefit in post-operative AF
- Inconsistent benefit in chronic AF
Key Point
- Not recommended solely for AF prevention
- Useful when there is coexisting CAD / dyslipidemia
4. Omega-3 Fatty Acids
Mechanisms
- Anti-inflammatory
- Stabilize atrial cell membranes
Evidence
- Mixed and largely negative
- No consistent benefit in AF prevention
❌ Not recommended routinely
5. Anti-Inflammatory Strategies
- Colchicine
- Corticosteroids (short-term)
Evidence
- Useful mainly in:
- Post-operative AF
- Post-ablation inflammation
6. Weight Reduction & Lifestyle Modification
(Arguably the most powerful upstream therapy)
Components
- Weight loss
- Exercise
- BP control
- Glycemic control
- Treatment of OSA
- Alcohol reduction
Evidence
- LEGACY trial
- ARREST-AF trial
✅ Reduces:
- AF burden
- AF progression
- Ablation recurrence
7. Treatment of Obstructive Sleep Apnea
- CPAP therapy
- Reduces nocturnal AF triggers
- Improves ablation outcomes
What Is NOT Upstream Therapy?
- Beta-blockers
- Calcium channel blockers
- Antiarrhythmic drugs
- Electrical cardioversion
(These are downstream rhythm or rate control)
Clinical Utility
Best Indications
- Primary prevention of AF
- Early AF
- Hypertension, HF, LVH
- Post-cardiac surgery
- Post-AF ablation substrate modification
Limited Role
- Long-standing persistent AF
- Advanced atrial fibrosis
Exam Pearls
- RAAS inhibitors = cornerstone
- Upstream therapy works best before AF is established
- Lifestyle modification > drugs
- Statins: post-operative AF benefit
- Omega-3: inconsistent / negative
- AF progression = failure of upstream control
One-Line Summary
Upstream therapy targets the atrial disease that causes AF, not the arrhythmia itself.
100 HARD, exam-oriented FAQs with concise but explanatory answers on
Upstream Therapy for Atrial Fibrillation, written at NEET-SS / INI / DM / cardiology fellowship level.
The questions deliberately target mechanisms, trials, pitfalls, and clinical reasoning, not definitions.
🔹 CORE CONCEPTS (1–10)
1. What exactly differentiates upstream from downstream AF therapy?
Upstream therapy modifies the atrial disease substrate (fibrosis, inflammation, stretch), whereas downstream therapy targets the electrophysiological expression (rate/rhythm).
2. Why is upstream therapy considered disease-modifying?
Because it alters structural remodeling pathways that drive AF initiation and progression, not just arrhythmia manifestation.
3. What does “AF begets AF” mechanistically mean?
AF induces electrical remodeling (shortened ERP) and structural remodeling (fibrosis), which further stabilize AF circuits.
4. Why does upstream therapy work best early in AF?
Early AF has reversible remodeling; late AF has fixed fibrosis.
5. Can upstream therapy terminate AF episodes?
No. It prevents occurrence or progression, not acute termination.
6. Is upstream therapy a replacement for antiarrhythmics?
No. It is adjunctive, not substitutive.
7. Why is atrial fibrosis central to AF pathophysiology?
Fibrosis causes conduction heterogeneity, reentry, and wavebreaks.
8. What atrial feature best predicts upstream therapy success?
Low fibrosis burden, often assessed by LGE-CMR or surrogates.
9. Why is left atrium the primary target, not ventricles?
AF is sustained by atrial substrate abnormalities, independent of ventricular myocardium.
10. Does CHA₂DS₂-VASc predict upstream therapy response?
No. It predicts stroke risk, not substrate reversibility.
🔹 RAAS INHIBITION (11–30)
11. Why does RAAS activation promote AF?
Angiotensin II stimulates fibroblast proliferation and collagen deposition.
12. What molecular pathway links RAAS to fibrosis?
Angiotensin II → TGF-β activation → collagen synthesis.
13. Which patients benefit MOST from ACEI/ARB therapy?
Hypertension, LVH, HF, and no prior AF (primary prevention).
14. Why is RAAS blockade less effective in permanent AF?
Fibrosis is already established and irreversible.
15. Which trial demonstrated AF reduction with losartan?
The LIFE trial.
16. Why are ARBs often superior to beta-blockers for AF prevention in HTN?
They reduce fibrosis, not just heart rate.
17. Do ACE inhibitors reduce AF recurrence after cardioversion?
Only modestly, mainly in patients with structural heart disease.
18. Are RAAS inhibitors useful post-ablation?
Yes, to reduce ongoing substrate progression.
19. Why does RAAS inhibition improve atrial conduction?
By reducing collagen barriers between myocytes.
20. Is RAAS inhibition effective in lone AF?
Limited benefit unless occult fibrosis or stretch exists.
21. Why does aldosterone worsen AF substrate?
It directly promotes myocardial fibrosis and inflammation.
22. Which RAAS component is most profibrotic?
Aldosterone > Angiotensin II.
23. Why are MRAs considered upstream therapy?
They directly block aldosterone-mediated fibrosis.
24. In which population are MRAs most useful?
Heart failure (HFrEF and HFpEF).
25. Can RAAS inhibitors reverse established fibrosis?
They may slow or partially regress early fibrosis, not advanced scar.
26. Why is RAAS inhibition considered primary prevention therapy?
It prevents new-onset AF, more than recurrent AF.
27. Does blood pressure reduction alone explain AF benefit?
No—fibrosis reduction is independent of BP lowering.
28. Are ACEI and ARB interchangeable for AF prevention?
Broadly yes; ARBs often better tolerated.
29. Do ARNIs have upstream AF benefit?
Likely yes via potent antifibrotic effects, but AF-specific data are evolving.
30. Why is RAAS blockade cornerstone upstream therapy?
It targets the central fibrosis pathway in AF.
🔹 STATINS & INFLAMMATION (31–45)
31. Why is inflammation important in AF pathogenesis?
Inflammation promotes atrial fibrosis and electrical instability.
32. How do statins act as upstream therapy?
Through anti-inflammatory and antioxidant effects, not lipid lowering.
33. In which AF setting are statins most effective?
Post-operative AF.
34. Why is post-operative AF inflammation-driven?
Surgical trauma, oxidative stress, and cytokine release.
35. Why are statins inconsistent in chronic AF prevention?
Chronic AF is fibrosis-dominant, not inflammation-dominant.
36. Are statins recommended solely for AF prevention?
No.
37. Which patients gain dual benefit from statins?
AF patients with CAD or dyslipidemia.
38. Do statins reduce AF burden post-ablation?
Marginal benefit, mostly early recurrence reduction.
39. Why do CRP levels correlate with AF incidence?
CRP reflects systemic inflammation driving atrial remodeling.
40. Why are corticosteroids not long-term upstream therapy?
Unacceptable side-effect profile.
41. What is colchicine’s role in AF?
Short-term inflammation suppression post-surgery or ablation.
42. Why is colchicine not routine upstream therapy?
Limited evidence outside specific inflammatory contexts.
43. Is AF an inflammatory disease?
Partly—especially in early or secondary AF.
44. Can inflammation alone sustain AF?
No; fibrosis is required for maintenance.
45. Why is inflammation considered an early AF driver?
It precedes fibrotic remodeling.
🔹 OMEGA-3 & FAILED THERAPIES (46–55)
46. Why were omega-3 fatty acids hypothesized to prevent AF?
Membrane stabilization and anti-inflammatory effects.
47. Why did omega-3 trials fail?
Insufficient substrate modification and inconsistent dosing.
48. Are omega-3s harmful in AF?
No, but ineffective for prevention.
49. What lesson do omega-3 failures teach?
Upstream therapy must significantly alter fibrosis, not minor biology.
50. Why do antioxidants generally fail in AF prevention?
Oxidative stress is secondary, not primary.
51. Can vitamin D prevent AF?
No consistent evidence.
52. Why do “nutraceuticals” fail as upstream therapy?
AF substrate disease is too advanced for weak interventions.
53. Is magnesium upstream therapy?
No—electrophysiologic, not disease-modifying.
54. Why is digoxin not upstream therapy?
It affects AV nodal conduction only.
55. Why do calcium channel blockers not qualify?
They do not modify atrial structure.
🔹 LIFESTYLE & RISK FACTOR MODIFICATION (56–75)
56. Why is weight loss the most powerful upstream therapy?
It reduces atrial stretch, inflammation, and fibrosis simultaneously.
57. Which trial established weight loss as AF therapy?
LEGACY.
58. Why is weight loss effect dose-dependent?
Greater weight loss → greater atrial reverse remodeling.
59. Why does obesity promote AF?
Epicardial fat, inflammation, atrial dilation.
60. Why is epicardial fat arrhythmogenic?
Paracrine cytokine release affecting atrial myocardium.
61. What is the role of exercise in upstream therapy?
Moderate exercise reduces AF; extreme endurance may increase AF.
62. Why is alcohol reduction crucial?
Alcohol directly promotes atrial fibrosis and triggers AF.
63. Why does “holiday heart” support upstream concepts?
Acute triggers act on vulnerable substrate.
64. Why is OSA one of the strongest AF drivers?
Intermittent hypoxia, negative intrathoracic pressure, sympathetic surges.
65. How does CPAP reduce AF recurrence?
Reduces nocturnal atrial stretch and autonomic instability.
66. Why does untreated OSA cause ablation failure?
Continued substrate progression.
67. Why is BP control upstream therapy?
Reduces atrial pressure and remodeling.
68. Why is glycemic control relevant?
Diabetes accelerates fibrosis.
69. Can lifestyle therapy reverse AF?
It can reduce burden and progression, rarely cure permanent AF.
70. Why is lifestyle therapy underutilized?
Delayed benefits and low patient adherence.
71. Is lifestyle therapy more effective than drugs?
Yes, in long-term AF burden reduction.
72. Should lifestyle therapy be first-line in early AF?
Yes.
73. Why does risk factor clustering accelerate AF?
Synergistic remodeling effects.
74. Is bariatric surgery upstream therapy?
Indirectly yes, via profound weight reduction.
75. Why is lifestyle therapy considered “foundational”?
All pharmacologic upstream therapies depend on it.
🔹 CLINICAL APPLICATION & EXAM TRAPS (76–100)
76. Can upstream therapy replace anticoagulation?
Never.
77. Does sinus rhythm restoration mean substrate reversal?
No.
78. Why does AF recur despite rhythm control?
Underlying substrate persists.
79. Which AF patients should NOT rely on upstream therapy alone?
Symptomatic or high-risk patients.
80. Why is long-standing persistent AF resistant?
Extensive fibrosis and electrical uncoupling.
81. What imaging best assesses AF substrate?
LGE-CMR.
82. Why is LA size an imperfect marker?
Fibrosis can exist without dilation.
83. Why do upstream therapies reduce AF progression but not eliminate AF?
They slow disease, not reverse scars.
84. Why is early diagnosis critical?
Earlier substrate modification is possible.
85. Why does AF progression predict worse outcomes?
More fibrosis → stroke, HF, mortality.
86. Should upstream therapy be started after first AF episode?
Yes, if risk factors exist.
87. Why do guidelines underemphasize upstream therapy?
Evidence heterogeneity and long timelines.
88. Why is HFpEF closely linked to AF?
Both are fibrosis-dominant diseases.
89. Why is AF considered a marker of atrial cardiomyopathy?
It reflects underlying atrial disease.
90. Can AF exist without atrial disease?
Rarely.
91. Why is AF recurrence after cardioversion common?
Substrate remains untreated.
92. Why do antiarrhythmics fail long-term?
They do not alter disease biology.
93. Why is combined upstream + downstream therapy optimal?
Symptom control + disease modification.
94. What single upstream intervention gives maximum benefit per effort?
Weight loss.
95. Why is AF management shifting toward upstream concepts?
Recognition of AF as chronic atrial disease.
96. Why is AF a progressive disorder?
Self-perpetuating remodeling.
97. What defines upstream therapy failure?
Continued AF progression despite risk control.
98. Why must upstream therapy be lifelong?
Substrate disease is chronic.
99. What is the exam-ready one-line summary?
“Treat the atrium, not just the rhythm.”
100. Ultimate principle of upstream therapy?
AF prevention = atrial disease prevention.
CASE-BASED VIVA QUESTIONS WITH MODEL ANSWERS on Upstream Therapy for Atrial Fibrillation, structured exactly as used in DM / DNB / NEET-SS / INI / fellowship oral exams.
Each case tests conceptual depth, mechanism, and decision-making, not rote facts.
🧠 CASE 1: Hypertensive Patient, No AF Yet
Case:
A 58-year-old man with long-standing hypertension and LVH on echo has no history of AF. ECG is normal.
Viva Questions
Q1. Does this patient have a risk for AF despite no arrhythmia yet?
Answer: Yes. Hypertension and LVH promote atrial stretch and fibrosis—key AF substrates.
Q2. Would you initiate upstream therapy here?
Answer: Yes. This is primary prevention, where upstream therapy works best.
Q3. Which drug class is most appropriate?
Answer: ACE inhibitor or ARB.
Q4. Why not a beta-blocker alone?
Answer: Beta-blockers control rate but do not reduce fibrosis.
Q5. What trial supports this approach?
Answer: LIFE trial—losartan reduced new-onset AF compared to atenolol.
🧠 CASE 2: Paroxysmal AF, Obese Patient
Case:
A 45-year-old obese man (BMI 34) with paroxysmal AF, structurally normal heart.
Viva Questions
Q6. What is the dominant AF driver here?
Answer: Obesity-related atrial stretch, inflammation, and epicardial fat.
Q7. What is the single most effective upstream therapy?
Answer: Weight loss.
Q8. Which trial supports this?
Answer: LEGACY trial.
Q9. Would you start antiarrhythmic drugs first?
Answer: No—risk-factor modification should be first-line.
Q10. What happens if obesity is untreated?
Answer: AF progression despite drugs or ablation.
🧠 CASE 3: Long-Standing Persistent AF
Case:
A 72-year-old woman with AF for 6 years, enlarged LA, failed cardioversion twice.
Viva Questions
Q11. Will upstream therapy restore sinus rhythm?
Answer: No.
Q12. Why is upstream therapy less effective here?
Answer: Advanced, irreversible atrial fibrosis.
Q13. Should upstream therapy still be continued?
Answer: Yes, to slow further progression, not to reverse AF.
Q14. Which investigation predicts poor response?
Answer: LGE-CMR showing extensive atrial fibrosis.
Q15. Key exam phrase?
Answer: “Upstream therapy works best before AF becomes permanent.”
🧠 CASE 4: Post-CABG AF
Case:
A 66-year-old man develops AF on day 3 after CABG.
Viva Questions
Q16. What is the dominant mechanism of AF here?
Answer: Acute inflammation and oxidative stress.
Q17. Which upstream therapy has strongest evidence?
Answer: Statins.
Q18. Why not RAAS inhibitors alone?
Answer: Acute inflammation dominates over fibrosis.
Q19. What adjunct therapy may help short-term?
Answer: Colchicine.
Q20. Is this AF likely to become chronic?
Answer: Usually no, if inflammation resolves.
🧠 CASE 5: AF with Heart Failure (HFpEF)
Case:
A 68-year-old woman with HFpEF and recurrent AF.
Viva Questions
Q21. Why is AF common in HFpEF?
Answer: Both are fibrosis-dominant diseases.
Q22. Which upstream drugs are most useful?
Answer: RAAS inhibitors and MRAs.
Q23. Why are MRAs particularly helpful?
Answer: Aldosterone strongly promotes atrial fibrosis.
Q24. Is rhythm control alone sufficient?
Answer: No—substrate modification is mandatory.
Q25. Exam pearl?
Answer: “HFpEF + AF = fibrosis problem.”
🧠 CASE 6: AF After Successful Ablation
Case:
A 52-year-old man, AF-free 6 months after ablation.
Viva Questions
Q26. Is upstream therapy still needed?
Answer: Yes.
Q27. Why, if AF is gone?
Answer: Ablation treats triggers, not disease substrate.
Q28. Which upstream measures reduce recurrence?
Answer: Weight loss, BP control, OSA treatment.
Q29. What happens if upstream therapy is ignored?
Answer: Late AF recurrence.
Q30. Exam line?
Answer: “Ablation without upstream therapy is incomplete treatment.”
🧠 CASE 7: AF with Obstructive Sleep Apnea
Case:
A 50-year-old man with AF and untreated OSA.
Viva Questions
Q31. How does OSA promote AF?
Answer: Hypoxia, sympathetic surges, negative intrathoracic pressure.
Q32. Is CPAP upstream therapy?
Answer: Yes.
Q33. Effect of untreated OSA on ablation?
Answer: High recurrence rates.
Q34. What exam phrase applies?
Answer: “No CPAP → no durable rhythm control.”
Q35. Why is OSA often missed?
Answer: AF clinics focus on ECG, not sleep history.
🧠 CASE 8: AF with Normal LA Size
Case:
A patient with AF but normal LA dimensions.
Viva Questions
Q36. Does normal LA size exclude atrial disease?
Answer: No.
Q37. What pathology may still exist?
Answer: Atrial fibrosis.
Q38. Best test to detect it?
Answer: LGE-CMR.
Q39. Why is LA size an imperfect marker?
Answer: Fibrosis can precede dilation.
Q40. Exam trap?
Answer: “Normal LA ≠ healthy atrium.”
🧠 CASE 9: AF with Diabetes and Hypertension
Case:
A 60-year-old diabetic, hypertensive patient with new AF.
Viva Questions
Q41. Which comorbidity accelerates fibrosis most?
Answer: Diabetes.
Q42. Best upstream drug strategy?
Answer: RAAS blockade + strict metabolic control.
Q43. Why is glycemic control upstream therapy?
Answer: Hyperglycemia promotes collagen deposition.
Q44. Will rhythm control alone work?
Answer: Poorly, without risk-factor control.
Q45. Exam summary?
Answer: “Metabolic disease = atrial disease.”
🧠 CASE 10: Examiner’s Final Question
Q46. Can upstream therapy replace anticoagulation?
Answer: Never.
Q47. Can upstream therapy cure AF?
Answer: No—it slows or prevents progression.
Q48. When should upstream therapy start?
Answer: At first diagnosis—or even before AF onset.
Q49. Most powerful upstream intervention overall?
Answer: Weight loss.
Q50. One-line viva conclusion?
Answer:
👉 “Upstream therapy treats the atrium; downstream therapy treats the rhythm.”







