Types of Wolff–Parkinson–White (WPW) syndrome
Types of Wolff–Parkinson–White (WPW) syndrome, we usually classify them based on pathway location, ECG pattern, and arrhythmia mechanism.
🔹 1. Based on ECG Manifestation
- WPW Pattern
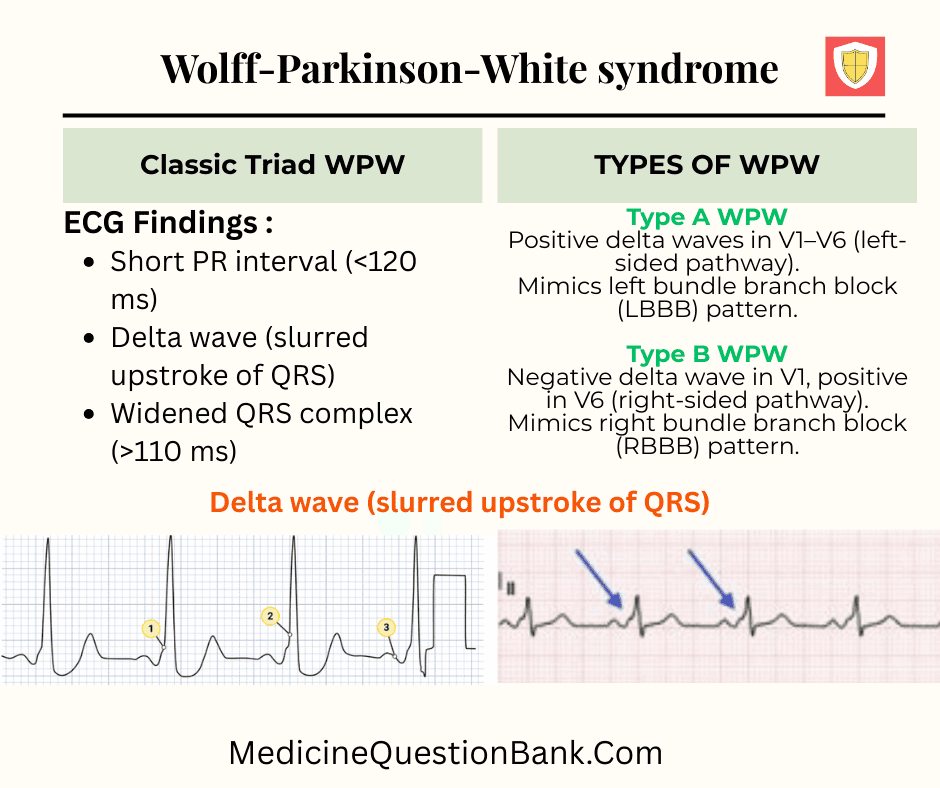
- ECG shows pre-excitation (short PR, delta wave, wide QRS)
- No clinical symptoms (incidental finding).
- WPW Syndrome
- ECG shows pre-excitation plus symptoms (palpitations, syncope, tachyarrhythmia).
🔹 2. Based on Pathway Location
- Left-sided WPW
- Accessory pathway on left atrioventricular ring.
- Most common (~50–60%).
- Right-sided WPW
- Accessory pathway on right AV ring (~30%).
- Septal WPW
- Midseptal, anteroseptal, or posteroseptal.
- Often multiple pathways and higher recurrence after ablation.
🔹 3. Based on ECG Pre-excitation Patterns
- Type A WPW
- Positive delta waves in V1–V6 (left-sided pathway).
- Mimics left bundle branch block (LBBB) pattern.
- Type B WPW
- Negative delta wave in V1, positive in V6 (right-sided pathway).
- Mimics right bundle branch block (RBBB) pattern.
- Type C WPW (less common)
- Rare, with mixed features depending on pathway location.
🔹 4. Based on Arrhythmia Mechanism
- Orthodromic AVRT (most common)
- Impulse goes down AV node and back up accessory pathway.
- Narrow QRS tachycardia.
- Antidromic AVRT
- Impulse goes down accessory pathway and back up AV node.
- Wide QRS tachycardia.
- Pre-excited Atrial Fibrillation
- Dangerous – very rapid ventricular response, risk of VF.
✅ So, to summarize:
- WPW Pattern vs Syndrome (symptomatic vs asymptomatic)
- Type A vs Type B vs Type C (ECG-based)
- Left-sided, Right-sided, Septal (anatomical)
- Orthodromic, Antidromic, AF-related (arrhythmia mechanism)
WPW Syndrome — 20 MCQs (Types A, B, C)
Types of WPW Syndrome
| Type | Accessory Pathway Location | ECG Characteristics | Mimics | Clinical Notes |
|---|---|---|---|---|
| Type A WPW | Left-sided accessory pathway (commonly left free wall / left atrium to left ventricle) | Tall R waves in V1, predominantly upright QRS in V1, wide QRS with positive delta wave | Mimics Left Bundle Branch Block (LBBB) | More common; easier to recognize |
| Type B WPW | Right-sided accessory pathway (commonly right free wall / right atrium to right ventricle) | Dominant S wave in V1, negative or biphasic QRS in V1, wide QRS with negative delta wave | Mimics Right Bundle Branch Block (RBBB) | Can be confused with RBBB on ECG |
| Type C WPW (less common) | Posteroseptal or other unusual pathway locations | ECG pattern variable depending on site; delta waves may be less obvious | Mixed or atypical conduction abnormalities | Seen less frequently; requires EP study for localization |
✅ Key Point:
- Type A WPW → Left-sided pathway → Looks like LBBB.
- Type B WPW → Right-sided pathway → Looks like RBBB.
- Type C WPW → Variable / posteroseptal pathways → Atypical ECG.
Wolff–Parkinson–White syndrome, WPW syndrome, WPW pattern, Accessory pathway, Bundle of Kent, Pre-excitation syndrome, Short PR interval, Delta wave, Wide QRS complex, Type A WPW, Type B WPW, Type C WPW, Left-sided WPW, Right-sided WPW, Septal WPW, LBBB mimic, RBBB mimic, AV reentrant tachycardia, Orthodromic AVRT, Antidromic AVRT, Pre-excited atrial fibrillation, Supraventricular tachycardia, Ventricular fibrillation, Sudden cardiac death, Procainamide, Ibutilide, Avoid AV nodal blockers, Verapamil contraindication, Digoxin contraindication, Adenosine contraindication, Radiofrequency ablation, Catheter ablation, Electrophysiology study, Lown–Ganong–Levine syndrome, AV nodal reentrant tachycardia, Bundle branch block , Paroxysmal supraventricular tachycardia







