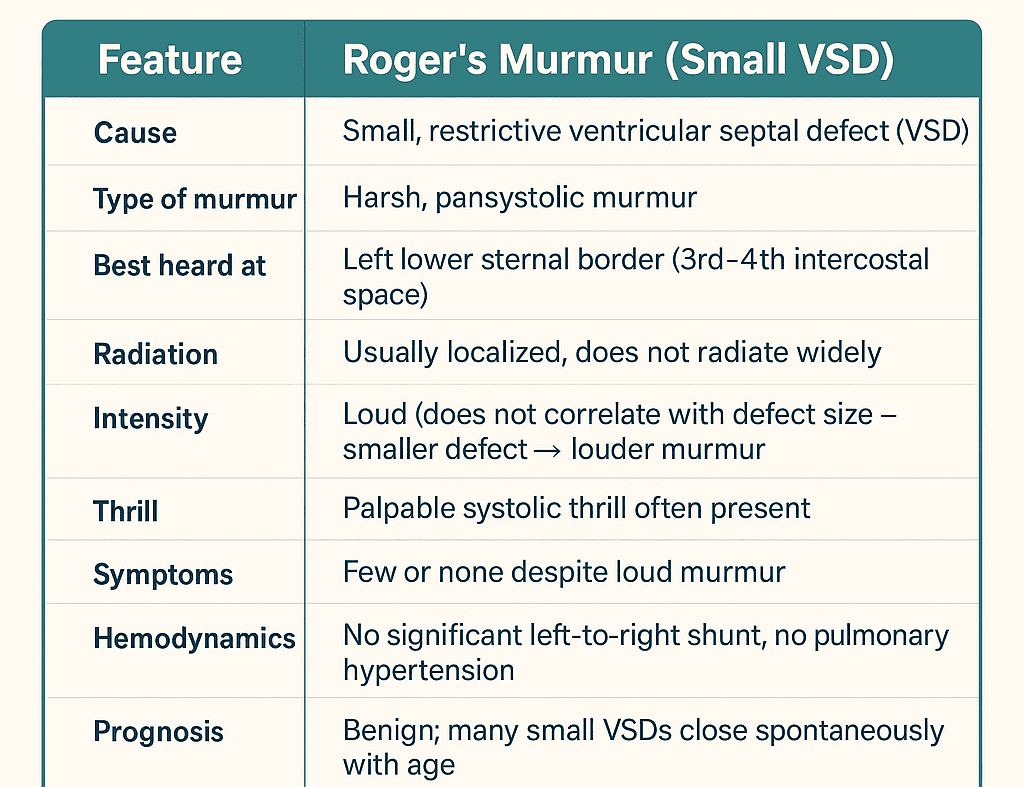
Left lower sternal border (3rd–4th intercostal space)
Radiation
Usually localized, does not radiate widely
Intensity
Loud (does not correlate with defect size – smaller defect → louder murmur)
Thrill
Palpable systolic thrill often present
Symptoms
Few or none despite loud murmur
Hemodynamics
No significant left-to-right shunt, no pulmonary hypertension
Prognosis
Benign; many small VSDs close spontaneously with age
Eponym
Named after Henri-Louis Roger (French physician)
Roger’s murmur is a classic pansystolic murmur associated with a small ventricular septal defect (VSD). Here’s a detailed explanation:
🔹 Key Features of Roger’s Murmur
Cause: Small, restrictive VSD (usually perimembranous or muscular).
Type: Harsh pansystolic murmur.
Best heard at:Left lower sternal border (3rd–4th intercostal space).
Radiation: Limited, usually does not radiate widely.
Intensity: Loud and harsh, often does not correlate with size of defect — smaller VSDs tend to produce louder murmurs (due to high-velocity jet across the narrow defect).
Thrill: Often associated with a palpable systolic thrill at the left sternal border.
Additional findings: Despite the loud murmur, the patient may have few or no symptoms (hence the paradox: loud murmur, but benign course).
🔹 Clinical Relevance
Named after Henri-Louis Roger, the French physician who first described it.
Commonly seen in children with small VSDs.
These patients often have normal growth and development, and the defect may close spontaneously with age.
No pulmonary hypertension or heart failure (unlike large VSDs).
🔹 Distinguishing Points
Loud murmur, minimal symptoms → hallmark of Roger’s murmur.
Small VSD → loud pansystolic murmur with thrill.
Large VSD → softer murmur, but more symptoms (dyspnea, heart failure, pulmonary hypertension).
Q1. Roger’s murmur is classically described as which type of murmur?
Best heard: LLSB
A. Harsh pansystolic murmur
B. Blowing systolic murmur
C. Diastolic decrescendo murmur
D. Continuous machinery murmur
Answer: A. Roger’s murmur is a harsh pansystolic murmur due to a small VSD, best heard at the left lower sternal border.
Q2. The loudness of Roger’s murmur typically correlates how with the size of the VSD?
A. Larger defect → louder murmur
B. Smaller (restrictive) defect → louder murmur
C. No relationship
D. Depends only on patient age
Answer: B. Restrictive (smaller) VSDs often produce higher-velocity jets and therefore louder murmurs (Roger’s murmur).
Q3. Where is Roger’s murmur best auscultated?
A. Right upper sternal border
B. Apex
C. Left lower sternal border (LLSB)
D. Left infraclavicular area
Answer: C. Roger’s murmur is classically loudest at the left lower sternal border (3rd–4th intercostal space).
Q4. A palpable systolic thrill is often present with Roger’s murmur. What does this indicate?
A. Severe pulmonary hypertension
B. Left ventricular failure
C. Aortic stenosis
D. High-velocity jet across a small VSD
Answer: D. A palpable thrill is due to the high-velocity jet across the small VSD producing turbulent flow.
Q5. Which of the following is TRUE about symptoms in patients with Roger’s murmur?
A. Often asymptomatic despite loud murmur
B. Always have heart failure
C. Always have growth failure in children
D. Frequently present with cyanosis
Answer: A. Many patients with a small VSD (Roger’s murmur) are asymptomatic and may have normal growth.
Q6. The murmur of a large VSD is usually which of the following compared with Roger’s murmur?
A. Louder and harsher
B. Softer despite larger defect
C. Changed to a diastolic murmur
D. Becomes continuous
Answer: B. Large VSDs often have softer murmurs since the pressure equilibrates between ventricles and velocity is lower.
Q7. Which ECG or clinical sign would be unlikely in an uncomplicated Roger’s murmur?
A. Normal growth and activity
B. No signs of heart failure
C. Significant pulmonary hypertension
D. Palpable thrill
Answer: C. Significant pulmonary hypertension is not typical in small restrictive VSDs producing Roger’s murmur.
Q8. Roger’s murmur is eponymously named after Henri-Louis Roger. Which specialty was he associated with?
A. Cardiac surgery
B. Pediatrics
C. Radiology
D. General medicine/physician
Answer: D. Roger was a 19th-century French physician; the eponym comes from his clinical descriptions.
Q9. Which hemodynamic feature explains the loud murmur in a small VSD?
A. High-velocity jet through a restrictive opening
B. Low-pressure gradient between ventricles
C. Continuous flow throughout systole and diastole
D. Left atrial enlargement
Answer: A. A small defect produces a high-velocity jet causing loud, harsh murmur and sometimes a thrill.
Q10. Which structural location is most commonly associated with VSDs producing Roger’s murmur?
A. Sinus venosus
B”>B. Perimembranous (membranous) region
C”>C. Ostium primum
D”>D. Patent ductus arteriosus
Answer: B. Many small VSDs are perimembranous (membranous) or muscular; perimembranous is common.
Q11. On auscultation, Roger’s murmur timing is:
A. Early diastolic
B. Continuous
C. Holosystolic / pansystolic
D. Mid-diastolic rumble
Answer: C. The murmur is pansystolic (holosystolic), heard throughout systole.
Q12. A loud pansystolic murmur with a thrill in an otherwise well child most likely suggests:
A. Small VSD with pulmonary hypertension
B. Large VSD causing heart failure
C. Isolated mitral regurgitation
D. Small restrictive VSD (Roger’s murmur)
Answer: D. A loud murmur with a thrill in an otherwise well child suggests a small restrictive VSD (Roger’s murmur).
Q13. Which investigation is most useful to confirm anatomic size and location of a VSD?
A. Transthoracic echocardiography (TTE)
B”>B. Chest X-ray
C”>C. ECG alone
D”>D. Cardiac enzymes
Answer: A. TTE is the investigation of choice to define size, location, and hemodynamic significance of a VSD.
Q14. Spontaneous closure of small VSDs is most likely during which period?
A. Late adulthood
B”>B. Early childhood / infancy
C”>C. After onset of pulmonary hypertension
D”>D. Never close spontaneously
Answer: B. Small VSDs commonly close spontaneously in infancy or early childhood.
Q15. Which complication is most associated with large, uncorrected VSDs rather than Roger’s murmur?
A. Palpable thrill without symptoms
B. Asymptomatic course
C. Eisenmenger syndrome (pulmonary vascular disease)
D. Spontaneous closure in infancy
Answer: C. Large VSDs can lead to significant left-to-right shunt and pulmonary vascular disease leading to Eisenmenger physiology if uncorrected.
Q16. Which auscultatory maneuver changes intensity of a VSD murmur (including Roger’s)?
A. Inspiration increases intensity
B. Handgrip increases intensity
C. Valsalva increases intensity
D. Generally little change with these maneuvers
Answer: D. Small VSD murmurs often change little with respiration or simple maneuvers; intensity is dominated by local jet velocity.
Q17. Which other murmur can mimic a pansystolic murmur at the LLSB?
A. Tricuspid regurgitation
B”>B. Aortic stenosis
C”>C. Mitral stenosis
D”>D. Patent ductus arteriosus
Answer: A. Tricuspid regurgitation causes a pansystolic murmur at the LLSB/left lower parasternal area and may mimic VSD.
Q18. Infective endocarditis risk in small restrictive VSDs (Roger’s murmur) is:
A. Extremely high and universal
B”>B. Increased compared to general population but low absolute risk
C”>C. Zero
D”>D. Only occurs after age 60
Answer: B. There is a slightly increased risk of endocarditis with VSDs compared with general population, but absolute risk is low.
Q19. In neonates, a loud pansystolic murmur suggests which of the following immediate steps?
A. Ignore and observe only
B”>B. Immediate cardiac surgery
C”>C. Prompt echocardiographic evaluation
D”>D. Start anticoagulation
Answer: C. A neonate with a loud murmur should have prompt echocardiography to define cardiac anatomy and hemodynamic significance.
Q20. Management of an asymptomatic child with a loud Roger’s murmur and small VSD usually includes:
A. Routine open-heart surgery
B”>B. Lifelong antibiotics
C”>C. Immediate catheter-based closure in all cases
D”>D. Clinical follow-up and echocardiographic monitoring; many small defects close spontaneously
Answer: D. Many small VSDs are managed conservatively with follow-up; intervention reserved for haemodynamically significant defects or complications.
Tip: Paste this full block into a WordPress HTML block. The script auto-initializes when the page loads. If your editor strips <script> tags, add the JS to your theme or a custom JS plugin and keep the HTML/CSS in the post.
✅ Summary: Roger’s murmur is a harsh pansystolic murmur at the left lower sternal border due to a small VSD, often with a thrill, loud in intensity, but paradoxically associated with few or no symptoms.
Roger’s murmur is
a loud, harsh, holosystolic heart murmur caused by a small ventricular septal defect (VSD), a congenital heart condition. The murmur is often compared to the sound of a “rushing waterfall” and is frequently accompanied by a palpable vibration known as a thrill.
Key characteristics
Cause: A VSD is a hole in the septum, or wall, that separates the two lower chambers (ventricles) of the heart. The size of the defect is a crucial factor: the smaller the defect, the more forceful the turbulent flow of blood and the louder the murmur.
Sound: The murmur is holosystolic (or pansystolic), meaning it persists throughout the entire ventricular contraction phase (systole). Its quality is typically harsh.
Location: The murmur is best heard at the left upper and lower sternal borders, and is often associated with a palpable thrill.
Symptom correlation: Henri-Louis Roger, the French pediatrician for whom the murmur is named, observed that patients with this loud murmur from a small VSD often have few to no symptoms. This contrasts with larger VSDs, which may produce a softer murmur but cause more significant hemodynamic issues and physical symptoms like shortness of breath.
Maladie de Roger
Roger’s murmur
The condition associated with a Roger’s murmur is sometimes referred to as maladie de Roger or Roger’s disease. This term describes a small, often asymptomatic VSD that is notable primarily for the loud murmur it produces. While this is a congenital heart disease, its prognosis is often good, as the small defect may close on its own, and the patient may not need intervention.