Rasmussen aneurysm
Rasmussen aneurysm
🩸 Rasmussen Aneurysm — Overview
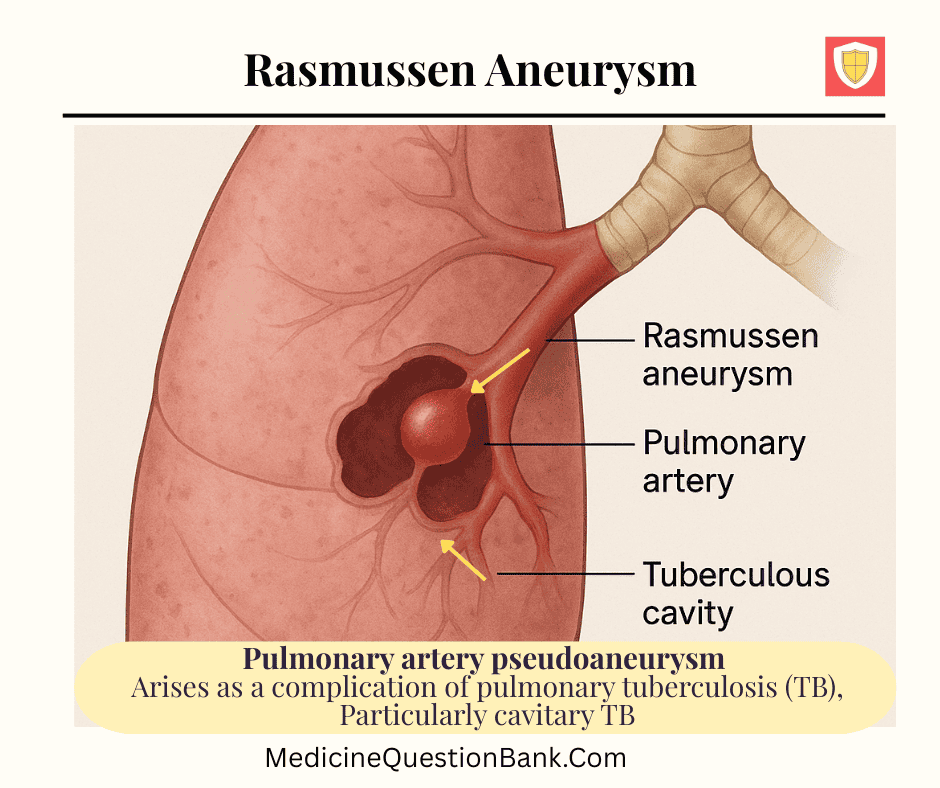
A Rasmussen aneurysm is a pulmonary artery pseudoaneurysm that arises as a complication of pulmonary tuberculosis (TB), particularly cavitary TB. It represents one of the classic causes of massive or life-threatening hemoptysis in TB patients.
🔬 Pathophysiology
- The inflammatory process from a tuberculous cavity extends into the adjacent pulmonary artery wall.
- This causes destruction of the arterial media and adventitia, leading to focal dilatation or pseudoaneurysm formation.
- The wall of the pseudoaneurysm is composed of inflammatory tissue and granulation, not all three arterial layers — hence a pseudoaneurysm.
🩻 Imaging Findings
1. CT Angiography (CTA):
- The gold standard for diagnosis.
- Shows a contrast-filled outpouching or enhancing focus within or adjacent to a tuberculous cavity.
- Typically located in the upper lobes (where cavitary TB is common).
2. Chest X-ray:
- May show a cavity but rarely demonstrates the aneurysm itself.
⚕️ Clinical Presentation
- Massive hemoptysis — can be sudden and fatal.
- Often in a patient with known pulmonary TB, especially with chronic cavitary disease.
- May be the initial presentation of previously undiagnosed TB in rare cases.
🩺 Differential Diagnosis of Massive Hemoptysis in TB
| Cause | Description |
|---|---|
| Rasmussen aneurysm | Erosion of pulmonary artery wall (pseudoaneurysm) |
| Bronchial artery hypertrophy/erosion | Most common overall cause of hemoptysis in TB |
| Aspergilloma | Fungal ball in an old TB cavity |
| Bronchiectasis | Post-TB fibrocavitary changes |
| Pulmonary infarction | Secondary to vasculitis or embolism |
🧠 Key Distinction
| Feature | True Aneurysm | Rasmussen Aneurysm (Pseudoaneurysm) |
|---|---|---|
| Wall composition | All 3 arterial layers | Fibrous tissue only |
| Stability | Relatively stable | Prone to rupture |
| Common vessels | Systemic or large arteries | Pulmonary arteries near cavities |
🧩 Management
- Urgent management is essential due to high mortality risk.
- Airway stabilization and control of bleeding.
- CT angiography to locate the bleeding site.
- Endovascular embolization of the affected pulmonary artery branch — treatment of choice.
- Antitubercular therapy (ATT) for underlying TB.
- Surgery (lobectomy/segmentectomy) only if embolization fails or not feasible.
💡 Key Takeaways
- Rasmussen aneurysm = Pulmonary artery pseudoaneurysm due to erosion from a tuberculous cavity.
- Massive hemoptysis may be the first clue.
- CT angiography is diagnostic.
- Endovascular embolization is the preferred management.
🩸 Rasmussen Aneurysm — 20 MCQs
1. Rasmussen aneurysm most commonly occurs as a complication of which disease?
2. Rasmussen aneurysm represents a pseudoaneurysm of which vessel?
3. The wall of a Rasmussen aneurysm is primarily composed of:
4. The most feared clinical manifestation of a Rasmussen aneurysm is:
5. Which imaging modality is most sensitive for diagnosing Rasmussen aneurysm?
6. Which lobe is most often affected by Rasmussen aneurysm?
7. Rasmussen aneurysm is classified as which type of aneurysm?
8. What is the preferred first-line management for a bleeding Rasmussen aneurysm?
9. In Rasmussen aneurysm, the arterial wall destruction is mainly due to:
10. Which of the following best describes the pathologic hallmark of Rasmussen aneurysm?
11. Which of the following is NOT a differential diagnosis for massive hemoptysis in TB?
12. Which statement about Rasmussen aneurysm is FALSE?
13. What is the main cause of death in patients with ruptured Rasmussen aneurysm?
14. In CT angiography, Rasmussen aneurysm appears as:
15. Which of the following treatments addresses the underlying cause?
16. Rasmussen aneurysm differs from a mycotic aneurysm because:
17. If embolization fails, the next best treatment is:
18. Which vessel type is most commonly the source of hemoptysis overall in TB?
19. On pathology, which feature distinguishes Rasmussen aneurysm?
20. Rasmussen aneurysm should always be suspected in a TB patient presenting with:
🩸 Rasmussen Aneurysm — Key Facts Table
| Definition | Rasmussen aneurysm is a pulmonary artery pseudoaneurysm that develops due to erosion of the arterial wall by a tuberculous cavity. |
|---|---|
| Etiology | Chronic pulmonary tuberculosis causing caseous necrosis and inflammation that weakens the adjacent pulmonary arterial wall. |
| Pathophysiology | Extension of infection from a cavity leads to destruction of the media and adventitia, replaced by granulation tissue → pseudoaneurysm formation. |
| Nature of aneurysm | Pseudoaneurysm (false aneurysm) — wall formed by granulation/inflammatory tissue, not the full arterial layers. |
| Common site | Upper lobes of the lungs (where cavitary TB is most common). |
| Clinical presentation | Massive hemoptysis (often sudden and life-threatening). May also present with cough and dyspnea if bleeding is slower. |
| Imaging findings |
|
| Differential diagnoses for hemoptysis in TB |
|
| Complication | Rupture → Massive airway bleeding → Asphyxiation and death. |
| Diagnosis | CT angiography is the gold standard; localizes bleeding and identifies pseudoaneurysm. |
| Management |
|
| Prognosis | Favorable if recognized early and embolized promptly. Mortality high in undiagnosed or ruptured cases. |
| Key differentiating point | Unlike true aneurysms, Rasmussen aneurysm lacks all three arterial layers — it is a pseudoaneurysm due to erosion by infection. |
| Historical note | Named after Danish pathologist Johan Nicolai Rasmussen (1840–1893), who first described this lesion in cavitary TB. |
🩸 Rasmussen Aneurysm — Related Terms & Concepts
| Primary Term | Rasmussen Aneurysm — Pulmonary artery pseudoaneurysm due to erosion from a tuberculous cavity. |
|---|---|
| Etiopathogenic Links |
|
| Associated Conditions |
|
| Radiologic/Diagnostic Terms |
|
| Interventional & Surgical Terms |
|
| Differential Diagnoses (Radiologic & Clinical) |
|
| Key Histopathologic Terms |
|
| Clinical Keywords |
|
| Relevant Radiologic Signs |
|
| Key Investigations |
|
| Related Eponyms / Historical Notes |
|
| Mnemonic (for recall) | “HEMOPTYSIS” mnemonic: H – Hemorrhage E – Erosion of pulmonary artery M – Massive bleeding O – Outpouching on CT P – Pulmonary artery pseudoaneurysm T – Tuberculosis cavity Y – Yields high mortality S – Stabilize airway I – Interventional embolization S – Start ATT |
A Rasmussen aneurysm is an inflammatory pseudoaneurysm—a leak in the artery wall contained by surrounding tissue—that develops on a branch of the pulmonary artery, typically as a rare complication of chronic, cavitary pulmonary tuberculosis. A rupture of this weakened vessel can cause severe, life-threatening internal bleeding.
Cause
Rasmussen aneurysms form as a result of chronic inflammation, most often from a tuberculous cavity eroding the adjacent pulmonary arterial wall. The inflammation leads to the destruction of the artery’s structural layers, weakening the wall and causing a contained rupture to form. While historically linked exclusively to tuberculosis, the term may now apply to similar aneurysms caused by other destructive lung diseases.
Symptoms
The most significant symptom of a Rasmussen aneurysm is hemoptysis (coughing up blood), which can range from mild and intermittent to massive and fatal. The massive bleeding from a ruptured aneurysm has a mortality rate as high as 50% if untreated. Other symptoms typically arise from the underlying infection, such as tuberculosis, and may include:
- Fever
- Cough
- Night sweats
- Shortness of breath
- Weight loss
Diagnosis
Because of the risk of massive hemorrhage, a timely and accurate diagnosis is critical, especially in patients with a history of tuberculosis.
- Computed Tomography (CT) Angiography: This is the primary diagnostic imaging tool. It can identify the aneurysm—which appears as a focal dilatation of a pulmonary artery branch—in or near a tuberculous lung cavity.
- Angiography: While more invasive, conventional angiography may be necessary for detailed evaluation, and can be performed concurrently with treatment.
Treatment
The main goal of treatment is to stop the bleeding and prevent a fatal rupture.
- Endovascular Embolization: The first-line and preferred treatment is a minimally invasive procedure called arterial transcatheter embolization. This procedure uses coils, glue, or other agents to block the blood supply to the aneurysm and stop the bleeding.
- Surgery: Surgical resection may be an option if embolization fails or is not appropriate.
- Anti-tuberculous Therapy: For mild bleeding, treatment of the underlying tuberculosis with anti-tuberculous medications can help resolve the hemoptysis.
This is for informational purposes only. For medical advice or a diagnosis, consult a professional. AI responses may include mistakes.
| Term | Explanation |
|---|---|
| Rasmussen Aneurysm | A pulmonary artery aneurysm adjacent to or within a tuberculous cavity. It occurs due to erosion of the pulmonary arterial wall by chronic inflammation, leading to hemoptysis (often massive). |
| Pulmonary Artery Aneurysm (PAA) | Abnormal focal dilation of a branch of the pulmonary artery. Can be congenital, post-stenotic, infectious, or inflammatory (like Rasmussen aneurysm). |
| Hemoptysis | Coughing up blood from the respiratory tract; in Rasmussen aneurysm, it results from rupture of the aneurysm into a cavity or bronchus. |
| Tuberculous Cavity | A caseating necrotic lesion formed in pulmonary tuberculosis; adjacent arteries may be eroded, predisposing to Rasmussen aneurysm. |
| Bronchial Artery Hypertrophy | Compensatory dilation of bronchial arteries in chronic infections like TB, which can also contribute to hemoptysis. |
| Mycotic Aneurysm | An infectious aneurysm caused by microbial invasion of an arterial wall (bacterial or fungal); Rasmussen aneurysm is a specific form of mycotic aneurysm due to Mycobacterium tuberculosis. |
| Pulmonary Angiography | Imaging technique used to visualize pulmonary arteries; helps confirm presence and location of Rasmussen aneurysm before embolization. |
| CT Pulmonary Angiogram (CTPA) | Preferred noninvasive test for detecting Rasmussen aneurysm; shows contrast-filled outpouching within or near a cavity. |
| Bronchial Artery Embolization (BAE) | Minimally invasive procedure to control hemoptysis by blocking bleeding vessels; may be required when Rasmussen aneurysm ruptures. |
| Pulmonary Tuberculosis (PTB) | Chronic granulomatous lung infection by Mycobacterium tuberculosis; responsible for cavitary lesions that predispose to Rasmussen aneurysm. |
| Cavity Wall Erosion | The mechanism by which arterial walls are weakened by inflammation and necrosis, leading to aneurysm formation. |
| Massive Hemoptysis | Life-threatening bleeding (>200–600 mL in 24 hours); Rasmussen aneurysm rupture is a key cause in TB-endemic regions. |
| Endovascular Embolization | Procedure to occlude aneurysm with coils or glue via catheter; the treatment of choice for Rasmussen aneurysm. |
| Pulmonary Arteriovenous Malformation (PAVM) | Abnormal direct connection between pulmonary arteries and veins; can mimic aneurysm radiologically but has different etiology. |
| Bronchopulmonary Anastomosis | Connection between bronchial and pulmonary arteries; becomes prominent in chronic inflammation, potentially worsening bleeding risk. |
| Pseudoaneurysm | Localized arterial dilatation with disruption of one or more vessel wall layers; Rasmussen aneurysm is a pseudoaneurysm. |
| Erosion Hemorrhage | Bleeding due to erosion of vessel wall by infection, tumor, or inflammation — mechanism in Rasmussen aneurysm. |
| Angiographic Coil Embolization | Placement of metallic coils into aneurysm to block blood flow and prevent rupture — standard therapy for Rasmussen aneurysm. |
| Contrast Extravasation | Leakage of contrast medium on CT indicating active bleeding, a key sign of a ruptured Rasmussen aneurysm. |
| Post-Tubercular Sequelae | Chronic changes such as fibrosis, bronchiectasis, or cavity formation after TB; can persist and predispose to late aneurysm formation. |
Rasmussen aneurysm, pulmonary artery pseudoaneurysm, tuberculosis aneurysm, hemoptysis in tuberculosis, pulmonary artery erosion, tuberculous cavity, mycotic aneurysm, CT pulmonary angiogram, bronchial artery embolization, pulmonary angiography, endovascular embolization, pulmonary tuberculosis complications, massive hemoptysis, TB cavity aneurysm, lung aneurysm, pseudoaneurysm in TB, Rasmussen aneurysm treatment, Rasmussen aneurysm diagnosis, tuberculosis vascular complication, Rasmussen aneurysm pathophysiology







