Imaging of Vulnerable Plaque — Current Status
Imaging of Vulnerable Plaque — Current Status
1. What Is a “Vulnerable Plaque” (Concept Update)
A vulnerable plaque is biologically active and rupture-prone, not merely stenotic.
Hallmark features
- Thin-cap fibroatheroma (TCFA) (<65 µm cap)
- Large lipid/necrotic core
- Positive (outward) remodeling
- Inflammation (macrophage-rich)
- Microcalcifications
- Endothelial dysfunction
⚠️ Key modern concept:
Patient vulnerability and plaque burden predict events better than identifying a single “dangerous” plaque.
2. Invasive Imaging Modalities (Current Gold Standards)
A. IVUS (Intravascular Ultrasound)
What it detects
- Plaque burden
- Positive remodeling
- Large lipid pools (indirect)
Key evidence
- PROSPECT trial: Plaque burden ≥70% + MLA ≤4 mm² → future events
Limitations
- Cannot directly visualize thin fibrous cap
- Poor for inflammation
Current role
- Risk stratification, not plaque rupture prediction
- Widely used, guideline-accepted
B. OCT (Optical Coherence Tomography) ⭐
Best modality for TCFA
What it detects
- Fibrous cap thickness (gold standard)
- Plaque rupture, erosion
- Macrophage accumulations
- Microchannels
Evidence
- CLIMA study: TCFA + macrophages + lipid arc → ↑ events
Limitations
- Limited penetration
- Requires contrast
- Focal, not whole-vessel
Current status
- Best available clinical tool to identify vulnerable morphology
- Still no indication to preemptively stent based on OCT alone
C. NIRS–IVUS (Near-Infrared Spectroscopy)
What it detects
- Lipid core burden index (LCBI)
Key trial
- PROSPECT II: High LCBI plaques predict events
Limitation
- Events driven by overall plaque burden, not single plaques
Status
- Promising, adjunctive
- Not guideline-mandated
3. Non-Invasive Imaging (Risk, Not Rupture)
A. Coronary CT Angiography (CCTA) ⭐⭐
High-risk plaque features
- Low attenuation plaque (<30 HU)
- Napkin-ring sign
- Positive remodeling
- Spotty calcification
Evidence
- SCOT-HEART, PROMISE: High-risk plaque → ↑ MACE
Limitation
- Cannot assess cap thickness
- Poor temporal resolution for rupture
Current role
- Best non-invasive tool for plaque vulnerability assessment
- Risk stratification, preventive intensification
B. PET Imaging (FDG / NaF)
What it detects
- Inflammation (FDG)
- Microcalcification (NaF)
Status
- Strong biological signal
- Research only
- Limited spatial resolution for coronaries
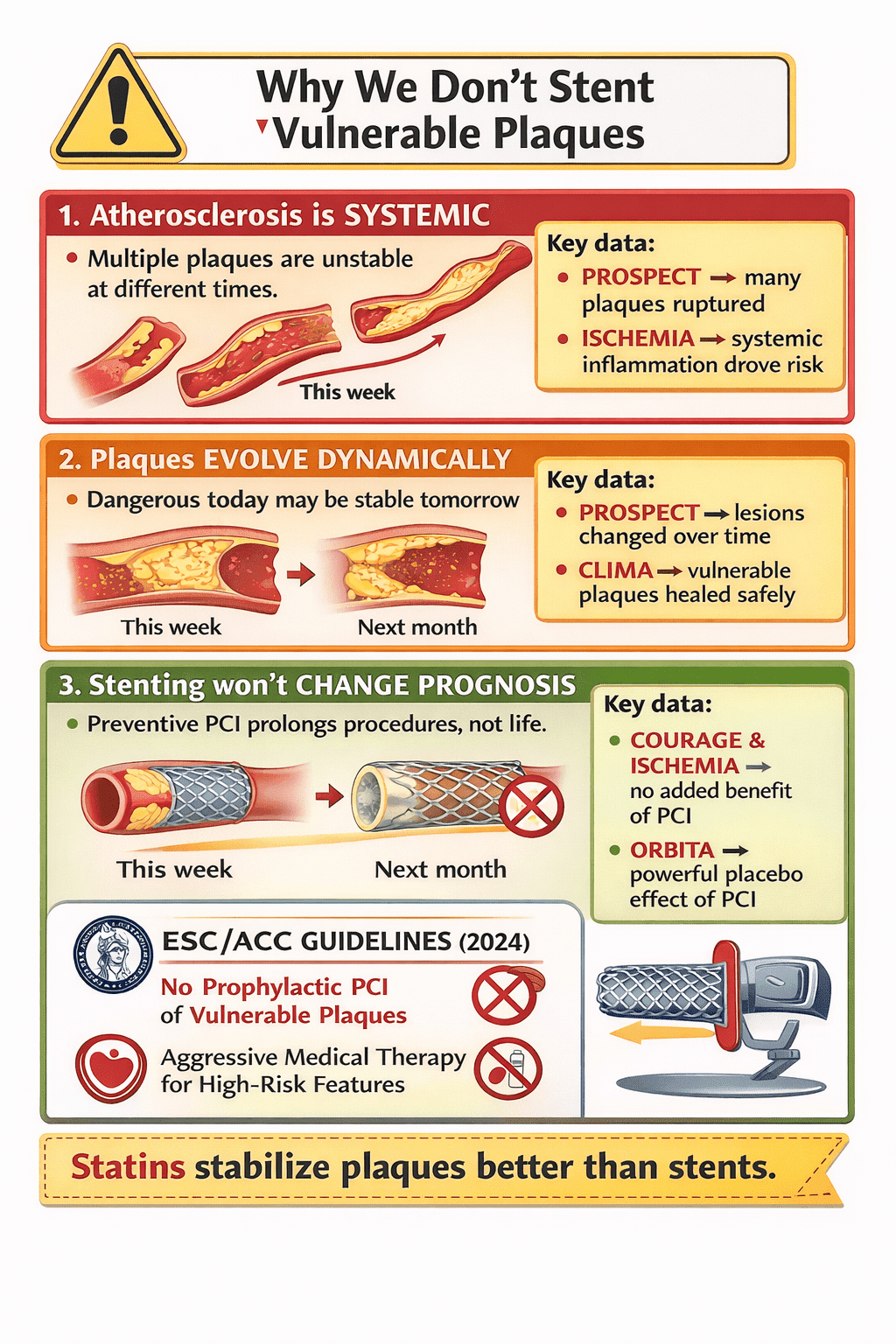
4. Why Vulnerable Plaque Imaging Has NOT Changed Therapy
Failed expectation:
“Identify the plaque → stent it → prevent MI”
Why this failed:
- Most MIs arise from non-obstructive plaques
- Plaques evolve dynamically
- Multiple plaques rupture silently
- Systemic inflammation > focal anatomy
Key message from PROSPECT & ISCHEMIA
Treat the patient, not the plaque
5. Current Guideline Position (ACC / ESC)
What is ACCEPTED
- IVUS / OCT for PCI optimization
- CCTA for risk stratification
- Aggressive medical therapy for high-risk plaque features
What is NOT recommended
- Prophylactic PCI of vulnerable plaques
- Routine invasive imaging solely to find TCFA
6. Practical Clinical Takeaways (Exam Gold)
| Question | Correct Answer |
|---|---|
| Best modality to detect TCFA | OCT |
| Best non-invasive risk marker | CCTA high-risk plaque features |
| Trial proving plaque burden matters | PROSPECT |
| Why plaque imaging failed to change outcomes | Systemic disease, not focal lesion |
| Management of vulnerable plaque | Aggressive medical therapy |
7. One-Line Exam Pearls
- OCT visualizes vulnerability, not actionability
- Vulnerable plaque ≠ vulnerable patient
- Statins stabilize plaques better than stents
- Imaging predicts risk, not rupture timing
🧠 Vulnerable Plaque Imaging + Trials — 80 SS One-Liners
Core Concepts
- Vulnerable plaque refers to biological instability, not angiographic severity.
- Most myocardial infarctions arise from non–flow-limiting plaques.
- Plaque burden predicts events better than single plaque morphology.
- Vulnerable plaque ≠ vulnerable patient.
- Atherosclerosis is a systemic inflammatory disease, not focal stenosis.
IVUS-Based Insights
- IVUS cannot directly visualize fibrous cap thickness.
- Plaque burden ≥70% on IVUS predicts future events (PROSPECT).
- Minimal luminal area ≤4 mm² increases risk but lacks specificity.
- IVUS identifies positive remodeling, a high-risk feature.
- IVUS-guided PCI improves stent optimization, not plaque prevention.
OCT-Specific Pearls
- OCT is the gold standard for fibrous cap thickness.
- Thin-cap fibroatheroma is defined as cap thickness <65 µm.
- OCT best identifies plaque rupture and erosion.
- Macrophage signal on OCT indicates inflammation.
- OCT penetration depth is inferior to IVUS.
OCT + Trials
- CLIMA study linked TCFA + macrophages + lipid arc to higher MACE.
- OCT-detected vulnerable plaques frequently heal spontaneously.
- No trial supports prophylactic PCI based on OCT findings alone.
- OCT vulnerability does not mandate intervention.
- OCT is diagnostic, not directive.
NIRS / Hybrid Imaging
- NIRS detects lipid-rich plaques via lipid core burden index (LCBI).
- LCBI ≥400 is considered high risk.
- NIRS does not assess cap thickness.
- PROSPECT II validated lipid-rich plaques as risk markers.
- Event rates correlated more with global disease burden than focal plaques.
CCTA (Non-Invasive Gold Standard)
- CCTA identifies high-risk plaque features non-invasively.
- Low attenuation plaque (<30 HU) predicts ACS.
- Napkin-ring sign indicates necrotic core with thin cap.
- Spotty calcification reflects active inflammation.
- Positive remodeling on CT indicates plaque vulnerability.
CCTA + Trials
- SCOT-HEART linked CT-detected high-risk plaques to future MI.
- PROMISE showed CT improves risk stratification, not outcomes alone.
- CT plaque features guide intensity of preventive therapy.
- CT cannot directly visualize fibrous cap thickness.
- CCTA is the best population-level vulnerability tool.
PET and Molecular Imaging
- FDG-PET identifies plaque inflammation.
- NaF-PET detects microcalcification activity.
- Coronary PET imaging is limited by spatial resolution.
- PET plaque imaging remains research-only.
- No PET-guided intervention strategy has proven outcome benefit.
Why Vulnerable Plaque Stenting Failed
- Most plaques that rupture were previously angiographically mild.
- Vulnerable plaques evolve dynamically over weeks to months.
- Many plaques rupture silently without causing MI.
- PCI treats anatomy, not inflammation.
- Treating one plaque ignores systemic disease.
Landmark Trials
- PROSPECT showed future events arise from non-culprit lesions.
- PROSPECT did not support preemptive stenting.
- ISCHEMIA showed no mortality benefit of routine invasive strategy.
- COURAGE demonstrated PCI does not reduce death or MI in stable CAD.
- ORBITA highlighted placebo effect of PCI in stable angina.
Guideline Position (ESC/ACC)
- No guideline recommends routine imaging to detect vulnerable plaques.
- Prophylactic PCI of vulnerable plaques is Class III (harm/no benefit).
- Invasive imaging is recommended for PCI optimization only.
- CCTA high-risk plaque warrants aggressive medical therapy, not PCI.
- Imaging informs risk, not rupture timing.
Management Implications
- Statins reduce lipid core volume and inflammation.
- High-intensity statins promote plaque stabilization.
- PCSK9 inhibitors reduce lipid-rich plaque burden.
- Anti-inflammatory therapy targets patient vulnerability.
- Medical therapy stabilizes plaques better than stents.
Exam Traps & Pearls
- The most dangerous plaque is often the least obstructive.
- Vulnerable plaque imaging predicts who, not when.
- OCT vulnerability ≠ indication for PCI.
- Plaque morphology does not equal clinical instability.
- Treating ischemia ≠ treating vulnerability.
High-Yield Summary Lines
- Vulnerable plaques are common; MI is rare.
- Systemic inflammation drives events more than focal anatomy.
- Imaging identifies risk, not destiny.
- The future is patient-level risk modification, not lesion-level stenting.
- Vulnerable plaque imaging refined prevention, not intervention.
Viva / SS Final Killers
- Best modality for TCFA: OCT.
- Best non-invasive vulnerability assessment: CCTA.
- Trial proving plaque burden matters: PROSPECT.
- Trial disproving routine PCI benefit: ISCHEMIA.
- Therapy of choice for vulnerable plaque: Statins + risk factor control.
Final Takeaways
- Vulnerable plaque detection has not changed revascularization strategy.
- PCI treats flow limitation, not plaque biology.
- Imaging is a risk amplifier, not a treatment trigger.
- The future lies in systemic anti-atherosclerotic therapy.
- Do not stent vulnerability—stabilize it.
| Feature | IVUS | OCT | NIRS (± IVUS) | CCTA |
|---|---|---|---|---|
| Modality | Invasive ultrasound | Invasive light-based | Invasive spectroscopy | Non-invasive CT |
| Resolution | Moderate (100–150 µm) | Highest (10–20 µm) | Chemical (no structure) | Moderate |
| Penetration depth | Deep (4–8 mm) | Shallow (1–2 mm) | NA | Full vessel wall |
| Fibrous cap thickness | ❌ No | ✅ Gold standard | ❌ No | ❌ No |
| Lipid core detection | Indirect | Indirect | ✅ Direct (LCBI) | Indirect (low HU) |
| Inflammation | ❌ Poor | ⚠️ Macrophage signal | ❌ No | ❌ No |
| Remodeling | ✅ Yes | Limited | ❌ No | ✅ Yes |
| Calcification | Good (extent) | Excellent (microcalcification) | ❌ No | Good |
| Whole-vessel assessment | ❌ Limited | ❌ Limited | ❌ Limited | ✅ Yes |
| Contrast required | ❌ No | ✅ Yes | ❌ No | ✅ Yes |
| PCI guidance | ✅ Excellent | ✅ Excellent | ❌ No | ❌ No |
| Vulnerable plaque detection | ⚠️ Indirect | ✅ Best morphology | ✅ Lipid risk marker | ✅ Risk features |
What Each Modality Is BEST For (Exam-Focused)
IVUS
- Plaque burden quantification
- Positive remodeling
- PCI optimization
- Key trial: PROSPECT
- Limitation: Cannot see fibrous cap
👉 Predicts risk via plaque burden, not rupture
OCT ⭐
- Thin-cap fibroatheroma (TCFA)
- Plaque rupture vs erosion
- Macrophage accumulation
- Stent edge/apposition details
- Key trial: CLIMA
👉 Best tool to DEFINE vulnerability, not to TREAT it
NIRS (± IVUS)
- Lipid Core Burden Index (LCBI ≥400)
- Identifies lipid-rich plaques
- Key trial: PROSPECT II
👉 Chemical risk marker without structural detail
CCTA ⭐⭐
- Non-invasive high-risk plaque features
- Low attenuation plaque
- Napkin-ring sign
- Spotty calcification
- Positive remodeling
- Key trials: SCOT-HEART, PROMISE
👉 Best population-level vulnerability assessment
Vulnerable Plaque Detection — Ranking (Exam)
| Feature | Best Modality |
|---|---|
| Fibrous cap thickness | OCT |
| Lipid core chemistry | NIRS |
| Plaque burden | IVUS |
| Non-invasive risk stratification | CCTA |
| PCI optimization | IVUS / OCT |
Why NONE of These Justify Preventive PCI
- Vulnerable plaques are dynamic
- Multiple plaques rupture silently
- Most MI plaques were non-obstructive
- Events correlate with systemic inflammation, not focal anatomy
Key trials teaching this lesson
- PROSPECT
- ISCHEMIA
- COURAGE
Guideline Position (ACC / ESC – Exam Line)
- ❌ No modality recommended to screen and stent vulnerable plaques
- ✅ IVUS / OCT recommended for PCI optimization only
- ✅ CCTA used for risk stratification and prevention intensification
One-Line Exam Killers
- IVUS sees burden, OCT sees cap, NIRS sees lipid, CT sees risk
- OCT predicts vulnerability, statins prevent MI
- Imaging identifies who is at risk, not which plaque to stent
- Treat the patient, not the plaque







