Erythropoietin Resistance index
Erythropoietin Resistance index
The erythropoietin resistance index (ERI) is
a formula used to evaluate the effectiveness of erythropoiesis-stimulating agents (ESAs) in treating anemia, particularly in patients with chronic kidney disease (CKD). A higher ERI indicates that a patient requires a larger dose of ESA to achieve a target hemoglobin level, suggesting a reduced response or “resistance” to the medication.
ERI calculation
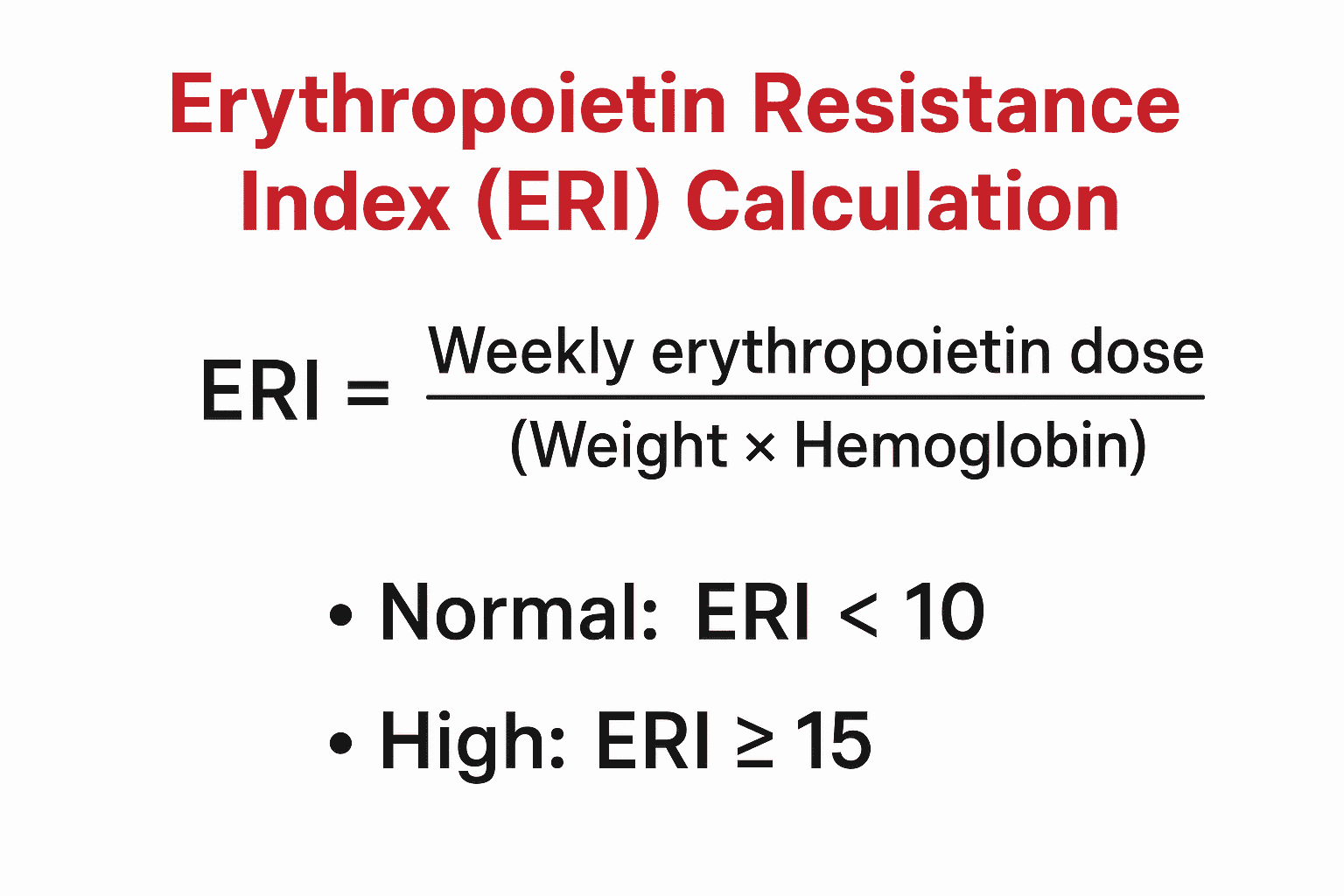
The specific formula for the ERI can vary slightly depending on the unit of measurement used for hemoglobin, but it is generally calculated as follows:
Erythropoietin Resistance Index (ERI) — 20 Interactive MCQs
1. Which of the following best defines the Erythropoietin Resistance Index (ERI)?
2. ERI units are most commonly expressed as:
3. Which formula is the correct algebraic form for ERI?
4. A higher ERI value indicates:
5. Which clinical situation commonly increases ERI (makes patients more ESA-resistant)?
6. Iron deficiency affects ERI how?
7. Which lab marker is most useful to investigate a high ERI?
8. Which of the following is a modifiable cause of an elevated ERI in dialysis patients?
9. For a 70-kg hemodialysis patient receiving 9000 IU epo per week with Hb 9 g/dL, ERI (IU/kg/week/g/dL) is approximately:
10. Which strategy is LEAST likely to reduce ERI?
11. Which statement about ERI and outcomes is correct?
12. Which of these interventions might be used when ERI remains high despite correcting iron deficiency?
13. Which patients most commonly have ERI monitoring as part of routine care?
14. A reasonable interpretation: ERI trending upward over weeks suggests:
15. Which medication class can blunt erythropoietin effect and raise ERI?
16. When calculating ERI you must ensure the weekly ESA dose is expressed in the same units. Which is TRUE?
17. A patient on darbepoetin uses µg dosing. To include darbepoetin in ERI, you should:
18. In research, why is ERI a useful metric?
19. Which of the following is a high-priority next step for a patient with rising ERI and low TSAT?
20. A pragmatic ERI threshold often used in studies to define ESA hyporesponsiveness (approximate and variable) is:
Significance of a high ERI
A high ERI is not just a laboratory curiosity but an important clinical indicator associated with a poorer prognosis in hemodialysis (HD) patients.
Clinical studies have shown that patients with a higher ERI often have an increased risk of:
- All-cause mortality: Research has consistently found a positive association between high ERI and an increased risk of death in HD patients.
- Cardiovascular mortality: A high ERI has also been linked to a higher risk of death from cardiovascular causes.
- Increased morbidity: Beyond mortality, a high ERI is associated with increased hospitalizations and other negative outcomes.
Factors associated with increased ERI
Many factors can contribute to increased erythropoietin resistance, reflecting an underlying inflammatory and catabolic state. These include:
- Inflammation: This is a major cause of ESA resistance. Inflammatory markers such as C-reactive protein (CRP) are often elevated in patients with a high ERI. The inflammation is caused by various factors, including uremic toxins and poor dialysis quality.
- Iron deficiency: Both absolute and functional iron deficiency can cause ESA hyporesponsiveness, even with high ferritin levels. Inflammation-induced hepcidin can cause iron to be sequestered, making it unavailable for erythropoiesis.
- Malnutrition: Poor nutritional status, reflected by low serum albumin and creatinine levels, is associated with a higher ERI.
- Dialysis quality: Inadequate dialysis, measured by lower Kt/V (a measure of dialysis adequacy), is a risk factor for EPO resistance.
- Comorbidities: Conditions such as congestive heart failure and diabetes are linked with higher ERI levels. Recent studies also suggest that SARS-CoV-2 infection can cause a transient but significant increase in ERI in HD patients.
- Hormonal imbalances: Secondary hyperparathyroidism and other endocrine issues can impact the effectiveness of ESAs.
- Medications: Some drugs, like ACE inhibitors and ARBs, have been linked to higher ESA resistance.
ERI’s limitations as a standalone metric
While useful, the ERI has limitations as an independent measure of ESA resistance.
- Surrogate for ESA dose: The ERI is strongly correlated with the weight-adjusted ESA dose. Some studies argue that the ERI is primarily a reflection of the dose administered rather than a separate measure of “resistance,” and that high ESA dosage itself is associated with poor outcomes, confounding the interpretation of ERI values.
- Does not replace full assessment: For clinicians, evaluating a patient’s response to ESAs involves a comprehensive review of all factors contributing to anemia and ESA hyporesponsiveness, not just the ERI number.
1. What does the Erythropoietin Resistance Index (ERI) measure?
A. Weekly erythropoietin dose divided by weight and hemoglobin
B. Serum ferritin divided by EPO dose
C. Hematocrit × iron saturation
D. Weekly dialysis dose per body weight
Answer: A. ERI quantifies EPO dose requirements standardized by body weight and hemoglobin, indicating EPO responsiveness.
2. Typical unit for ERI is:
A. IU/m²
B. IU/kg/week/g/dL
C. µg/kg/day
D. mg/kg/hour
Answer: B. ERI is expressed as IU per kg body weight per week per g/dL of hemoglobin.
3. Formula for calculating ERI is:
A. Hb × weight / EPO dose
B. EPO dose × Hb / weight
C. ERI = EPO dose / (weight × Hb)
D. EPO dose / Hb only
Answer: C. ERI = weekly ESA dose / (weight × Hb).
4. A higher ERI implies:
A. High ESA sensitivity
B. Lower mortality risk
C. High iron saturation
D. ESA hyporesponsiveness or resistance
Answer: D. A high ERI denotes poor response to EPO (hyporesponsiveness).
5. Which condition commonly raises ERI?
A. Chronic inflammation
B. Adequate iron
C. Low CRP
D. High dialysis adequacy
Answer: A. Inflammation reduces EPO effectiveness and increases ERI.
6. Iron deficiency affects ERI by:
A. Decreasing ERI
B. Increasing ERI
C. No effect
D. Normalizing ERI
Answer: B. Iron deficiency blunts erythropoiesis, raising ERI.
7. Key lab markers to assess in a high ERI patient are:
A. ALT/AST
B. Sodium/potassium
C. Ferritin and TSAT
D. Amylase
Answer: C. Evaluate ferritin and TSAT to check for iron deficiency causing resistance.
8. Modifiable cause of high ERI is:
A. Age
B. Genetic factors
C. Diabetes duration
D. Iron deficiency
Answer: D. Iron deficiency is correctable and lowers ERI after treatment.
9. A 70-kg patient receives 9000 IU/week ESA with Hb 9 g/dL. ERI ≈ ?
A. 14.3 IU/kg/week/g/dL
B. 1.4 IU/kg/week/g/dL
C. 0.14 IU/kg/week/g/dL
D. 7 IU/kg/week/g/dL
Answer: A. 9000 ÷ (70×9) ≈ 14.3 IU/kg/week/g/dL.
10. Which action is least likely to reduce ERI?
A. Treat inflammation
B. Increase dialysate sodium
C. Give IV iron
D. Control hyperparathyroidism
Answer: B. Dialysate sodium changes don’t influence ERI directly.
🩸 Erythropoietin Resistance Index (ERI) – NEET PG Preparation
Erythropoietin Resistance Index (ERI) is an important topic for NEET PG, INI-CET, and USMLE aspirants. It helps assess how effectively patients with chronic kidney disease (CKD) respond to erythropoiesis-stimulating agents (ESAs). A high ERI indicates ESA hyporesponsiveness, often due to factors like iron deficiency, inflammation, or poor dialysis adequacy.
This interactive NEET PG quiz covers the definition, formula, normal values, causes, and clinical relevance of ERI in CKD anemia management. Practice these questions to strengthen your nephrology and hematology concepts for postgraduate entrance exams.







