Delirium
Delirium
Hallmark of delirium is a defcit of
[A] Attention
[B] Memory
[C] Visuospatial tasks [D] Language
Hallmark of delirium
Hallmark of delirium is a deficit of attention, although all cognitive domains—including memory,
executive unction, visuospatial tasks, and language— are variably involved.
Associated symptoms that may be present in some cases include altered sleep-wake cycles, perceptual disturbances such as hallucinations or delusions, a ect changes, and autonomic ndings that include heart rate and blood pressure instability.
primary hallmark of delirium is an acute, fluctuating disturbance in attention and awareness. This involves a reduced ability to direct, focus, sustain, or shift attention, often developing rapidly over hours to days.
Key Clinical Features
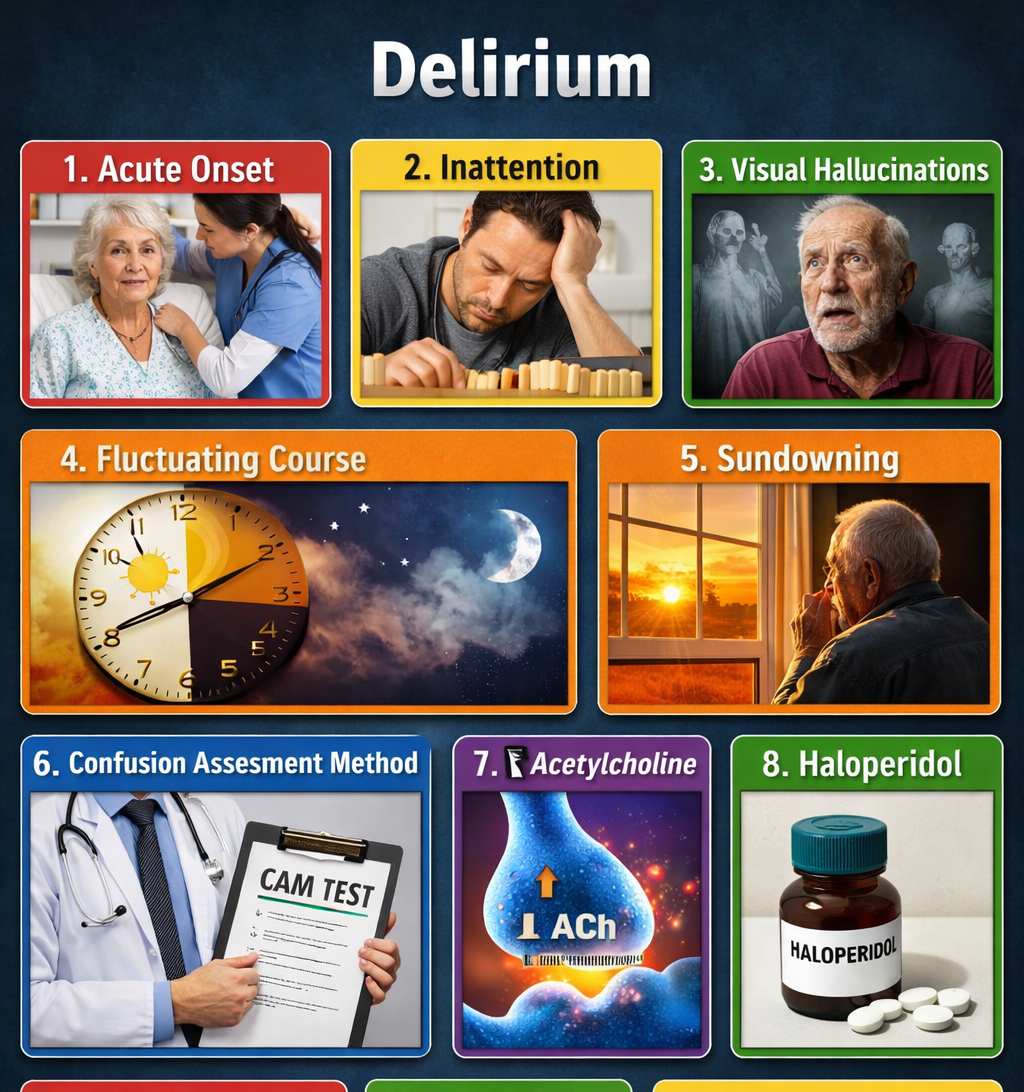
Medical professionals often look for four core features to diagnose delirium, notably used in the Confusion Assessment Method (CAM):
- Acute Onset and Fluctuating Course: Symptoms appear suddenly and often change in severity throughout the day, sometimes worsening at night—a phenomenon known as “sundowning”.
- Inattention: The person may be easily distracted or have significant trouble following a conversation or command.
- Disorganised Thinking: This manifests as incoherent, rambling, or nonsensical speech.
- Altered Level of Consciousness: This can range from hyperalertness and agitation to extreme drowsiness and lethargy.
Common Subtypes
Delirium is often categorized based on the patient’s activity level:
- Hyperactive: Characterized by restlessness, agitation, and sometimes hallucinations or delusions. It is often the easiest type to recognize.
- Hypoactive: The most common but frequently missed type, characterized by sluggishness, drowsiness, and withdrawal. It is often misidentified as depression.
- Mixed: Involves symptoms that fluctuate between the hyperactive and hypoactive states.
Distinguishing from Dementia
While both conditions involve confusion, they have distinct profiles:
| Feature | Delirium | Dementia |
|---|---|---|
| Onset | Sudden/Acute (hours to days) | Slow/Insidious (months to years) |
| Attention | Significantly impaired early on | Generally preserved until late stages |
| Course | Fluctuating (better/worse during the day) | Steady and progressive |
| Reversibility | Usually reversible if cause is treated | Nearly always irreversible |