Belhassen Ventricular Tachycardia (VT) is a rare idiopathic form of ventricular tachycardia that typically arises in structurally normal hearts, and is one of the “fascicular ventricular tachycardias.” It is sometimes called fascicular VT or verapamil-sensitive VT.
🔹 Key Features of Belhassen VT
Origin
Arises from the left posterior fascicle of the left bundle branch.
Re-entry mechanism involving the Purkinje system.
Typical ECG Findings
QRS morphology: Right bundle branch block (RBBB)-like pattern.
Axis: Left axis deviation (because it originates in the posterior fascicle).
Relatively narrow QRS for VT (110–140 ms).
Regular rhythm, rates usually 120–180 bpm.
Clinical Context
Seen in young, otherwise healthy patients.
Often precipitated by exercise, emotional stress, or catecholamine surge.
Not associated with structural heart disease (important differentiating point).
Pharmacological Response
Resistant to adenosine, lidocaine, and beta-blockers.
Sensitive to IV verapamil, which can terminate the tachycardia (hence “verapamil-sensitive VT”).
Treatment Options
Acute termination: IV verapamil.
Chronic management:
Catheter ablation has a high success rate (>90%), often curative.
Verapamil or beta-blockers may be used in patients not suitable for ablation.
Prognosis
Generally excellent in the absence of structural heart disease.
Not typically associated with sudden cardiac death (unlike other VTs).
🔹 Differentiating Belhassen VT from Other VTs
Typical VT: Wide QRS, often in structural heart disease, poor prognosis.
Belhassen VT: Narrower QRS, RBBB with LAD, no structural heart disease, verapamil-sensitive, good prognosis.
Q1. Belhassen VT typically occurs in patients with:
A. Structural heart disease
B. Healthy, structurally normal hearts
C. Prior myocardial infarction
D. Dilated cardiomyopathy
✅ It is an idiopathic VT, usually seen in young healthy hearts without structural disease.
Q2. The most common origin of Belhassen VT is:
A. Right ventricular outflow tract
B. Left posterior fascicle
C. Left anterior fascicle
D. AV node
✅ Classic Belhassen VT originates from the left posterior fascicle.
Q3. ECG in Belhassen VT usually shows:
A. Left bundle branch block with right axis deviation
B. Right bundle branch block with left axis deviation
C. Narrow QRS with normal axis
D. Polymorphic QRS
✅ The typical ECG shows RBBB morphology with left axis deviation.
Q4. The QRS width in Belhassen VT is usually:
A. >160 ms
B. 120–140 ms
C. <90 ms
D. >200 ms
✅ QRS complexes are relatively narrow for VT, typically 120–140 ms.
Q5. Belhassen VT is MOST sensitive to:
A. Adenosine
B. Amiodarone
C. Verapamil
D. Lidocaine
✅ Verapamil terminates Belhassen VT, hence called “verapamil-sensitive VT.”
Q6. Which of the following does NOT terminate Belhassen VT?
A. Verapamil
B. Adenosine
C. Catheter ablation
D. Electrical cardioversion
✅ Adenosine is ineffective in fascicular VT.
Q7. Typical heart rate in Belhassen VT is:
A. 60–100 bpm
B. 120–180 bpm
C. 200–240 bpm
D. >300 bpm
✅ Heart rate is usually moderate, 120–180 bpm.
Q8. The underlying mechanism of Belhassen VT is:
A. Triggered activity
B. Re-entry
C. Enhanced automaticity
D. Torsades de pointes
✅ It is due to a re-entrant circuit involving the fascicular Purkinje network.
Q9. Prognosis of Belhassen VT is generally:
A. Poor, with high risk of sudden death
B. Good, rarely life-threatening
C. Associated with severe LV dysfunction
D. Requires ICD in all patients
✅ Prognosis is excellent in the absence of structural heart disease.
Q10. Which acute therapy is MOST effective?
A. IV Verapamil
B. IV Adenosine
C. IV Lidocaine
D. IV Magnesium
✅ IV Verapamil is the drug of choice for acute termination.
Q11. Belhassen VT is most common in which age group?
A. Elderly with ischemic heart disease
B. Young adults
C. Infants
D. Post-menopausal women
✅ It usually presents in young, otherwise healthy adults.
Q12. Catheter ablation success rate in Belhassen VT is approximately:
A. 50%
B. 70%
C. >90%
D. <30%
✅ Catheter ablation has a very high success rate, over 90%.
Q13. In ECG, Belhassen VT shows:
A. RBBB pattern, LAD
B. LBBB pattern, RAD
C. QS in V1
D. Delta waves
✅ The hallmark is RBBB morphology with left axis deviation.
Q14. Belhassen VT is sometimes classified as:
A. RVOT tachycardia
B. Fascicular VT
C. AV nodal tachycardia
D. Bundle branch re-entry tachycardia
✅ Belhassen VT is a subtype of fascicular tachycardia.
Q15. Which class of drug is MOST effective?
A. Class IC
B. Class III
C. Non-dihydropyridine calcium channel blockers
D. Beta-blockers
✅ Non-dihydropyridine calcium channel blockers (verapamil, diltiazem) are effective.
Q16. Which diagnostic clue helps distinguish Belhassen VT from SVT with aberrancy?
A. Very wide QRS
B. Relatively narrow QRS with RBBB + LAD
C. Irregular rhythm
D. Variable AV conduction
✅ The combination of RBBB with LAD in a narrow VT favors fascicular VT.
Q17. Belhassen VT typically presents with:
A. Syncope and sudden cardiac death
B. Palpitations and mild dizziness
C. Recurrent angina
D. Pulmonary edema
✅ Most patients complain of palpitations or mild dizziness, rarely syncope.
Q18. Which of the following is TRUE?
A. Belhassen VT usually occurs during sleep
B. Triggered by exertion, stress, catecholamines
C. Always requires an ICD
D. Cannot be ablated
✅ It is often catecholamine-induced and may occur with exertion or stress.
Q19. Belhassen VT should be suspected when:
A. Polymorphic VT in structural heart disease
B. Young patient, RBBB + LAD, resistant to adenosine
C. Wide QRS tachycardia in MI
D. Irregular narrow QRS tachycardia
✅ Classic scenario: young, no structural disease, RBBB+LAD morphology, adenosine-resistant.
Q20. Long-term prognosis after catheter ablation in Belhassen VT is:
A. Poor
B. Excellent
C. Requires ICD backup
D. Variable with high recurrence
✅ Ablation is curative in most cases, with excellent long-term prognosis.
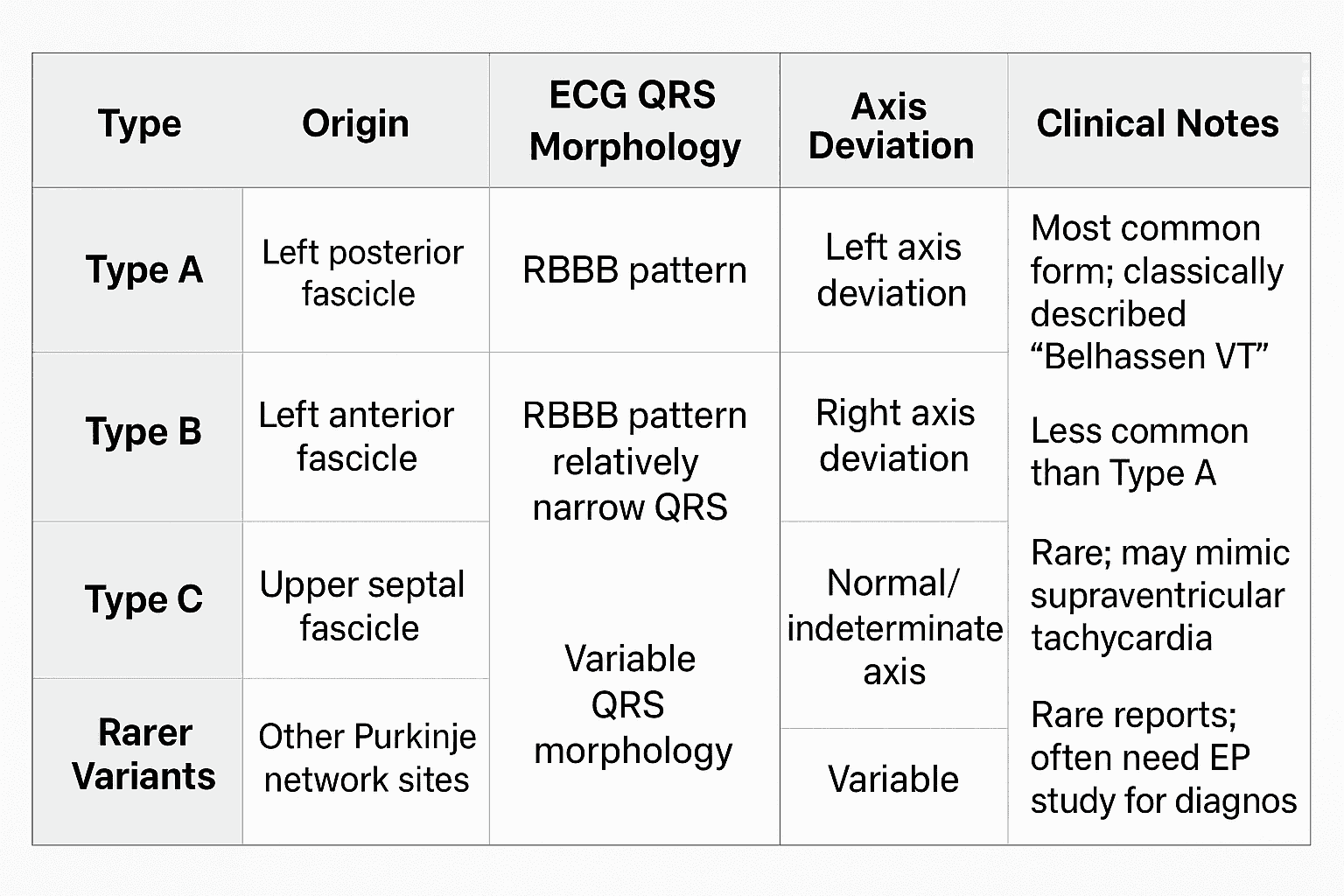
Type
Origin
ECG QRS Morphology
Axis Deviation
Clinical Notes
Type A
Left posterior fascicle
RBBB pattern
Left axis deviation
Most common form; classically described “Belhassen VT”
Type B
Left anterior fascicle
RBBB pattern
Right axis deviation
Less common than Type A
Type C
Upper septal fascicle
RBBB pattern, relatively narrow QRS
Normal/indeterminate axis
Rare; may mimic supraventricular tachycardia
Rarer Variants
Other Purkinje network sites
Variable QRS morphology
Variable
Rare reports; often need EP study for diagnosis
📌 Key points across all types:
Mechanism: Re-entry involving the Purkinje fibers
Verapamil-sensitive (terminates with IV verapamil)
Occurs in structurally normal hearts
Prognosis: Generally excellent
Catheter ablation is highly effective (>90% cure rate)
Belhassen ventricular tachycardia, fascicular VT, idiopathic VT, verapamil-sensitive VT, Type A fascicular VT, Type B fascicular VT, Type C fascicular VT, rare variants fascicular VT, left posterior fascicle VT, left anterior fascicle VT, upper septal fascicle VT, Purkinje fiber reentry, RBBB morphology, left axis deviation, right axis deviation, narrow QRS tachycardia, exercise-induced VT, stress-induced VT, catheter ablation, verapamil therapy, adenosine-resistant VT, structurally normal heart VT, idiopathic left ventricular tachycardia, ILVT, ECG features Belhassen VT, prognosis Belhassen VT.