ATRIAL FIBRILLATION (40 ADVANCED FAQs)
SS / DM CARDIOLOGY — ATRIAL FIBRILLATION (40 ADVANCED FAQs)
1. Why did EAST-AFNET 4 show benefit while AFFIRM did not?
Because rhythm control was initiated early (≤1 year of diagnosis), before atrial remodeling occurred, and anticoagulation was continued irrespective of rhythm.
2. Is rhythm control now superior to rate control in all AF patients?
No. Benefit is confined to early AF with cardiovascular comorbidity. Late or long-standing AF behaves like AFFIRM.
3. What is the most common misconception about rhythm control?
That restoration of sinus rhythm eliminates stroke risk. Stroke prevention is independent of rhythm strategy.
4. Why is lenient rate control (<110 bpm) acceptable?
RACE II showed no difference in mortality, HF, or stroke versus strict control, with fewer drugs and adverse effects.
5. When is strict rate control still preferred?
- Persistent symptoms
- Tachycardia-induced cardiomyopathy
- HFrEF with poor tolerance
6. Which NOAC demonstrated reduction in stroke, bleeding, and mortality?
Apixaban (ARISTOTLE trial).
7. Why can’t NOACs be used in moderate–severe mitral stenosis?
Because pivotal NOAC trials excluded rheumatic MS; warfarin remains standard.
8. Why was ROCKET-AF considered a “high-risk” trial?
Mean CHADS₂ ≈3.5, unlike ARISTOTLE/RE-LY (~2).
9. What made RE-LY methodologically unique?
Open-label warfarin with blinded dabigatran arms.
10. Which AF trial first showed mortality benefit of ablation?
CASTLE-AF, in HFrEF patients with ICD/CRT-D.
11. Why did CABANA fail to show superiority?
High crossover diluted intention-to-treat analysis.
12. When is catheter ablation first-line therapy?
- Symptomatic paroxysmal AF
- AF with HFrEF
- Early AF with high symptom burden
13. What is the “blanking period” after AF ablation?
First 3 months, during which AF recurrence does not equal failure.
14. Why does AV node ablation + CRT improve survival in permanent AF?
Eliminates irregularity and dyssynchrony, improving ventricular efficiency (APAF-CRT).
15. Why is AF with WPW dangerous?
Rapid conduction via accessory pathway → VF risk if AV nodal blockers are given.
16. Which drugs are contraindicated in AF with WPW?
- Digoxin
- Verapamil
- Diltiazem
- Beta-blockers
17. Preferred acute drug for AF with WPW (stable)?
IV procainamide.
18. Why does stroke risk peak days after cardioversion?
Due to atrial stunning and delayed recovery of mechanical function.
19. Minimum ECG duration to diagnose AF?
≥30 seconds (ESC definition).
20. What defines “valvular AF” today?
Only:
- Mechanical valve
- Moderate–severe mitral stenosis
21. Why is AF common in heart failure?
- Atrial stretch
- Neurohormonal activation
- Fibrosis → re-entry circuits
22. What is tachycardia-induced cardiomyopathy?
Reversible LV dysfunction caused by persistent rapid AF.
23. Best rate-control drug in HFrEF?
Beta-blocker ± digoxin
(avoid non-DHP CCBs).
24. When is digoxin preferred?
- Hypotension
- Sedentary patients
- As add-on therapy
25. Why does ibutilide cause torsades?
QT prolongation due to IKr blockade.
26. Preferred anticoagulant reversal agents?
- Dabigatran → Idarucizumab
- Factor Xa inhibitors → Andexanet alfa / PCC
27. Is CHA₂DS₂-VASc = 1 in men an indication for OAC?
Consider anticoagulation after shared decision-making.
28. Does female sex alone mandate anticoagulation?
No. It is a risk modifier, not an independent indication.
29. Why is aspirin ineffective in AF stroke prevention?
AF strokes are cardioembolic, not platelet-driven.
30. Best post-PCI regimen in AF with high bleeding risk?
NOAC + P2Y12 inhibitor, avoid aspirin (AUGUSTUS, PIONEER).
31. Why does OSA worsen AF?
Intermittent hypoxia → atrial remodeling and autonomic imbalance.
32. Does CPAP reduce AF recurrence?
Yes, significantly in observational and post-ablation studies.
33. ECG difference between AF and multifocal atrial tachycardia?
- AF: no P waves
- MAT: ≥3 different P-wave morphologies
34. What is “subclinical AF”?
AF detected on devices without symptoms, still stroke-relevant.
35. Does AF burden matter for anticoagulation?
Risk increases with duration, but CHA₂DS₂-VASc remains primary determinant.
36. Why is dronedarone contraindicated in severe HF?
ANDROMEDA showed increased mortality.
37. Can cardioversion be done without anticoagulation?
Only if:
- AF <48 hours and
- Low stroke risk
(Still controversial)
38. Why does AF cause irregular pulse deficit?
Variable AV nodal conduction → inconsistent ventricular filling.
39. When is left atrial appendage occlusion considered?
- High stroke risk
- Absolute contraindication to long-term OAC
40. Single most important principle in AF management?
Anticoagulation decisions override rhythm or rate strategy.
| Step | Domain | Key Decision Point | SS / DM–Level Details |
|---|---|---|---|
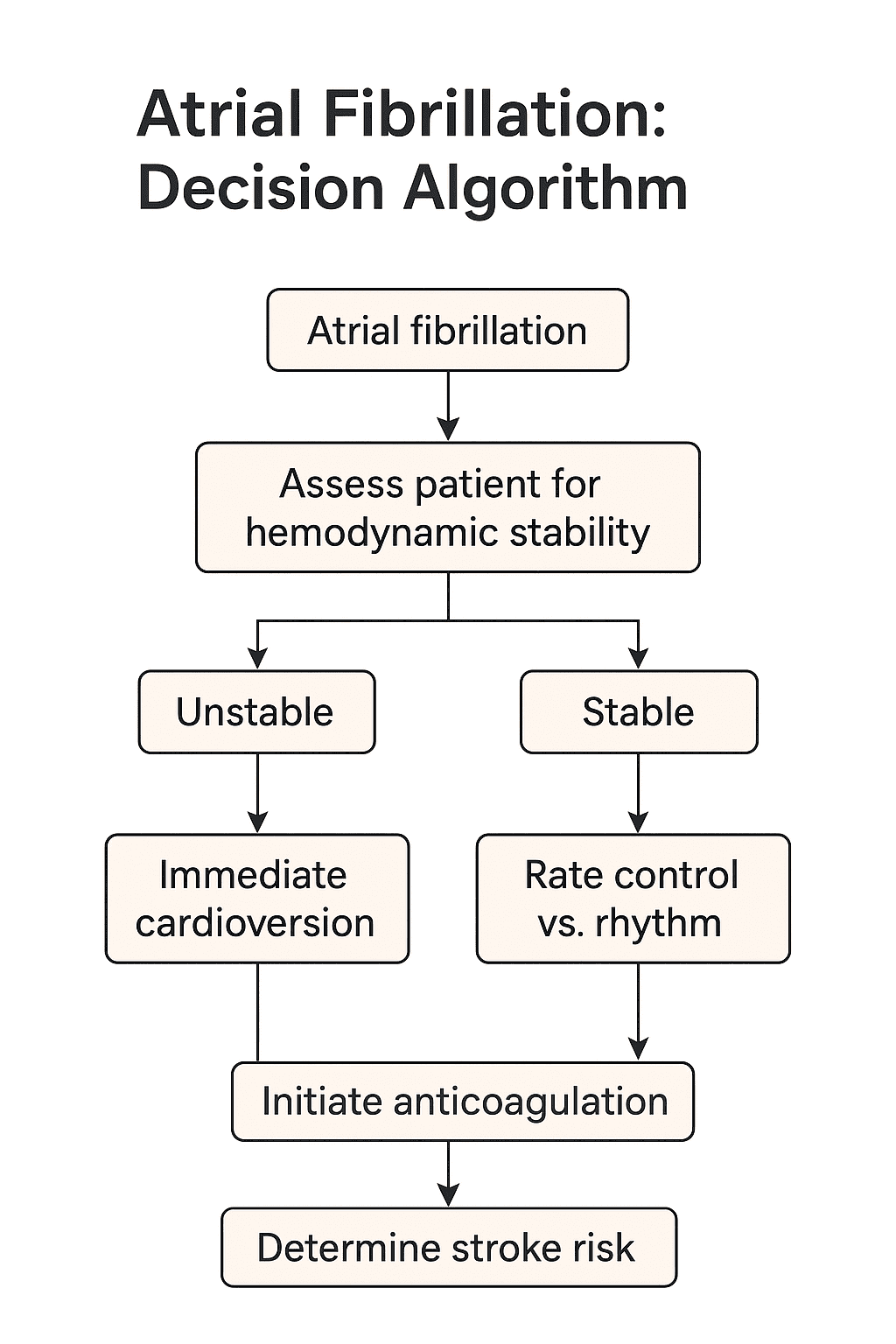
| 1 | Diagnosis | ECG criteria | Irregularly irregular RR interval + no discrete P waves, AF ≥ 30 sec |
| 2 | Stability | Hemodynamic status | Unstable = hypotension, shock, ischemia, pulmonary edema |
| 3 | Unstable AF | Immediate action | Synchronized DC cardioversion (anticoagulation not a prerequisite) |
| 4 | Stable AF | Initial strategy | Rate vs rhythm decided by symptoms, duration, LV function |
| 5 | Rate control | Target heart rate | Lenient <110 bpm (RACE II) unless symptomatic / TIC |
| 6 | Rate control drugs | Preserved EF | β-blocker or diltiazem/verapamil |
| 7 | Rate control drugs | HFrEF | β-blocker ± digoxin (avoid non-DHP CCBs) |
| 8 | Rhythm control | Ideal candidates | Early AF, symptomatic AF, HF, young patients |
| 9 | Rhythm drugs | Structural heart disease | Amiodarone |
| 10 | Rhythm drugs | No structural disease | Flecainide / propafenone |
| 11 | Ablation | First-line indication | Symptomatic paroxysmal AF, AF with HFrEF |
| 12 | Ablation benefit | Mortality data | CASTLE-AF showed ↓ mortality in HFrEF |
| 13 | Blanking period | Post-ablation | First 3 months — recurrence ≠ failure |
| 14 | Cardioversion | AF >48 hours | 3 weeks anticoagulation OR TEE-guided |
| 15 | Cardioversion | AF <48 hours | Can cardiovert; anticoagulation still advised |
| 16 | Stroke risk | Risk stratification | CHA₂DS₂-VASc |
| 17 | Anticoagulation | CHA₂DS₂-VASc ≥2 (men) | Mandatory OAC |
| 18 | Anticoagulation | CHA₂DS₂-VASc =1 (men) | Consider OAC (shared decision) |
| 19 | Valvular AF | Definition | Mechanical valve or moderate–severe MS |
| 20 | Valvular AF | Drug of choice | Warfarin only |
| 21 | Non-valvular AF | Preferred OAC | NOACs over warfarin |
| 22 | Best NOAC | Outcome profile | Apixaban (↓ stroke, bleeding, mortality) |
| 23 | AF + PCI | Antithrombotic strategy | NOAC + P2Y12 inhibitor (avoid aspirin) |
| 24 | AF + WPW | Contraindicated drugs | Digoxin, β-blockers, diltiazem, verapamil |
| 25 | AF + WPW | Acute stable therapy | IV procainamide |
| 26 | AF + HF | Rhythm benefit | Early rhythm control improves outcomes |
| 27 | TIC | Definition | LV dysfunction due to rapid AF — reversible |
| 28 | Digoxin | Best use case | Hypotension, sedentary patients |
| 29 | Dronedarone | Contraindication | Severe HF (ANDROMEDA ↑ mortality) |
| 30 | Stroke timing | Post-cardioversion | Highest risk due to atrial stunning |
| 31 | AF burden | Stroke relevance | Increases risk, but CHA₂DS₂-VASc dominates |
| 32 | Subclinical AF | Management | Anticoagulate based on risk score |
| 33 | OSA | AF recurrence | Treat with CPAP |
| 34 | LAA occlusion | Indication | High stroke risk + OAC contraindication |
| 35 | Rate vs rhythm | Core principle | Anticoagulation overrides strategy |
| 36 | Aspirin | Role | No role in AF stroke prevention |
| 37 | ECG differential | AF vs MAT | AF: no P waves; MAT: ≥3 P morphologies |
| 38 | Lenient rate | Trial | RACE II |
| 39 | Early rhythm | Trial | EAST-AFNET 4 |
| 40 | Final rule | Exam pearl | “Treat stroke risk first, rhythm later” |







