Methods to identify vulnerable plaque
Methods to identify vulnerable plaque.
Vulnerable plaque = an atherosclerotic plaque prone to rupture or erosion, leading to ACS. Identification relies on morphology, composition, inflammation, biomechanics, and biology. No single modality is definitive; multimodal assessment is often required.
1. Invasive Coronary Imaging (Gold-standard for morphology)
1. Intravascular Ultrasound (IVUS)
- Findings suggestive of vulnerability
- Large plaque burden (>70%)
- Positive (expansive) remodeling
- Attenuated plaque (lipid-rich)
- VH-IVUS: identifies thin-cap fibroatheroma (TCFA) pattern
- Limit: poor cap thickness resolution
2. Optical Coherence Tomography (OCT) (Best for fibrous cap)
- Highest axial resolution (~10–20 μm)
- Detects:
- Thin fibrous cap (<65 μm)
- Lipid-rich plaque (lipid arc >90°)
- Macrophage infiltration
- Microchannels, plaque rupture, erosion
- Current in-vivo gold standard for TCFA
3. Near-Infrared Spectroscopy (NIRS)
- Quantifies lipid burden
- Lipid Core Burden Index (LCBI)
- LCBI >400 → high-risk plaque
- Often combined with IVUS (NIRS–IVUS)
4. Coronary Angioscopy
- Direct visualization
- Yellow plaques = lipid-rich, vulnerable
- Limited availability; mainly research
2. Non-Invasive Coronary Imaging
5. Coronary CT Angiography (CCTA) (Most practical non-invasive tool)
High-risk plaque features:
- Low-attenuation plaque (<30 HU)
- Positive remodeling
- Napkin-ring sign
- Spotty calcification
Clinical value: predicts future ACS independent of stenosis severity
6. Cardiac MRI (CMR)
- Black-blood imaging for vessel wall
- Identifies:
- Lipid-rich necrotic core
- Intraplaque hemorrhage
- Limited spatial resolution for coronaries (better for carotids)
7. PET Imaging
- 18F-FDG → plaque inflammation (macrophages)
- 18F-NaF → active microcalcification (rupture-prone)
- Hybrid PET–CT / PET–MRI improves localization
3. Functional & Biomechanical Assessment
8. Endothelial Dysfunction
- Coronary vasomotor response to acetylcholine
- Dysfunction correlates with plaque vulnerability
9. Hemodynamic Forces
- Low endothelial shear stress (ESS) → plaque progression
- High ESS at cap shoulders → rupture risk
- Assessed via computational flow dynamics (research)
4. Circulating Biomarkers (Adjunctive)
10. Inflammatory Biomarkers
- hs-CRP
- IL-6
- MPO (myeloperoxidase)
11. Plaque Instability Markers
- MMPs (matrix metalloproteinases)
- Oxidized LDL
- Lp-PLA₂
(Not plaque-specific; risk stratification only)
5. Emerging / Experimental Techniques
- Molecular imaging of macrophages
- Targeted nanoparticles
- AI-based plaque phenotyping (CCTA + IVUS/OCT)
- Radiomics for CT plaque texture
Exam-Oriented Summary (NEET-SS / DM Cardiology)
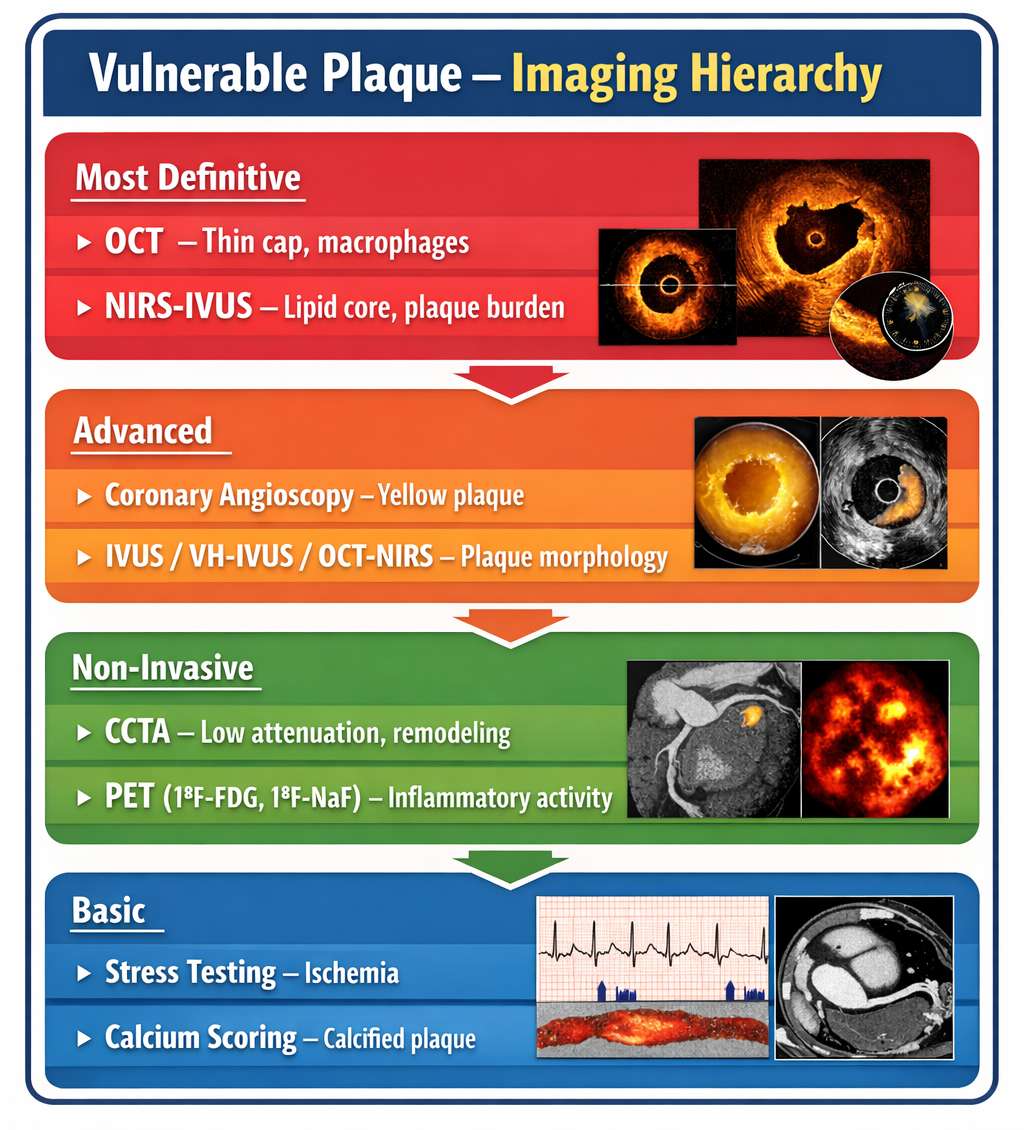
| Modality | Best Detects |
|---|---|
| OCT | Thin fibrous cap, macrophages (best overall) |
| NIRS | Lipid core burden |
| IVUS | Plaque burden, remodeling |
| CCTA | Non-invasive high-risk plaque features |
| PET (NaF) | Active microcalcification |
| Angioscopy | Yellow plaque |
Key Point: Vulnerable plaque ≠ flow-limiting stenosis. Most ACS arise from mild–moderate lesions.
1. The single most specific in-vivo criterion for defining TCFA is:
Only OCT-measured fibrous cap thickness <65 μm defines TCFA. Other features are supportive but non-definitive.
2. Which imaging modality has the highest spatial resolution for fibrous cap assessment?
OCT resolution is ~10–20 μm, far superior to IVUS (~100 μm).
3. Lipid Core Burden Index (LCBI) >400 is derived from:
NIRS quantifies lipid content and generates LCBI; >400 predicts future MACE.
4. Napkin-ring sign on CCTA represents:
Napkin-ring sign = low-attenuation core with peripheral higher attenuation rim → high-risk plaque.
5. Which PET tracer best identifies plaques prone to rupture rather than inflammation?
18F-NaF binds to microcalcification, indicating active plaque destabilization.
6. A plaque causing ACS despite <50% stenosis most commonly represents:
Most ACS arise from non-obstructive but vulnerable plaques.
7. Positive coronary remodeling on IVUS is defined as:
Positive (expansive) remodeling = lesion EEM area ÷ reference EEM area >1.05, associated with vulnerable plaques.
8. OCT feature most specific for plaque erosion rather than rupture is:
Plaque erosion shows intact cap with overlying thrombus, unlike rupture where cap disruption is seen.
9. Which combination best defines a high-risk plaque on CCTA?
Low-attenuation plaque with positive remodeling is the classic vulnerable plaque phenotype on CCTA.
10. Attenuated plaque on IVUS typically represents:
Attenuation without calcium shadowing on IVUS indicates lipid-rich vulnerable plaque.
11. Which modality directly visualizes plaque color?
Angioscopy shows yellow plaques, which correlate with lipid-rich vulnerable plaques.
12. Thin-cap fibroatheroma is MOST commonly detected in vivo by:
Only OCT can reliably measure fibrous cap thickness <65 μm in vivo.
13. Which plaque feature correlates BEST with inflammation?
Macrophage infiltration reflects active inflammation and plaque instability.
14. Low endothelial shear stress is associated with:
Low shear stress promotes plaque growth, while rupture often occurs at high shear regions.
15. Which PET tracer reflects macrophage metabolic activity?
18F-FDG uptake reflects inflammatory macrophage activity in plaques.
16. Spotty calcification on CCTA suggests:
Small, spotty calcifications are associated with rupture-prone plaques.
17. Which OCT feature predicts future ACS independently?
Fibrous cap thickness is a stronger predictor than angiographic severity.
18. NIRS falsely underestimates lipid when:
Calcium interferes with near-infrared signal penetration.
19. Plaque rupture most often occurs at:
High shear stress concentrates at plaque shoulders, predisposing to rupture.
20. Which biomarker best reflects plaque instability rather than burden?
MPO reflects oxidative stress and cap weakening.
21. In PROSPECT study, future events arose predominantly from lesions with:
PROSPECT showed non-obstructive plaques cause most future ACS.
22. Napkin-ring sign corresponds histologically to:
Peripheral higher attenuation reflects fibrous tissue surrounding lipid core.
23. Which is NOT a vulnerable plaque feature?
A thick cap implies plaque stability.
24. Best modality to detect intraplaque hemorrhage is:
CMR is superior for detecting intraplaque hemorrhage, especially in carotids.
25. Which lesion is MOST likely to cause sudden ACS?
Vulnerability, not stenosis severity, determines ACS risk.
26. OCT overestimates lipid when plaque contains:
Calcium causes signal attenuation mimicking lipid pools.
27. High-risk plaque progression is MOST associated with:
Low ESS promotes lipid accumulation and plaque growth.
28. Which combination best predicts plaque rupture?
Structural weakness plus lipid load defines rupture risk.
29. Which is TRUE regarding plaque erosion?
Plaque erosion often affects younger patients, smokers, and women.
30. Which imaging feature best correlates with future MACE?
TCFA presence strongly predicts adverse events.
31. IVUS limitation in vulnerable plaque detection is:
IVUS resolution is insufficient for thin fibrous cap measurement.
32. Which statement about vulnerable plaques is CORRECT?
Most vulnerable plaques are angiographically mild.
33. Best non-invasive predictor of vulnerable plaque is:
CCTA allows direct plaque morphology assessment.
34. Which feature indicates plaque stabilization?
Dense, confluent calcification is a marker of plaque healing.
35. Which combination is MOST dangerous?
Lipid burden plus structural weakness defines maximal vulnerability.
36. Which modality best integrates structure and composition?
Hybrid NIRS–IVUS provides plaque burden and lipid composition.
37. Vulnerable plaque concept emphasizes:
Plaque composition and inflammation drive ACS risk.
38. Which statement regarding calcium is TRUE?
Microcalcification causes local stress amplification, unlike dense calcium.
39. Ultimate clinical goal of vulnerable plaque detection is:
Identification aims at aggressive preventive therapy, not lesion counting.
40. The strongest predictor of future ACS among imaging features is:
Plaque composition and biology predict events better than stenosis severity.