High-Altitude Pulmonary Edema
High-Altitude Pulmonary Edema (HAPE)
High-Altitude Pulmonary Edema is a non-cardiogenic pulmonary edema that occurs in susceptible individuals after rapid ascent to high altitude, usually >2,500–3,000 m. It is one of the most serious forms of high-altitude illness and can rapidly become fatal if untreated.
1. Definition
HAPE is acute pulmonary edema caused by hypoxia-induced pulmonary hypertension and capillary leak at high altitude, occurring in individuals without primary cardiac disease.
2. Typical Altitude Risk
| Altitude | Risk |
|---|---|
| <2500 m | Rare |
| 2500–3000 m | Possible |
| >3000 m | Common in susceptible individuals |
| >4500 m | High risk |
Common locations:
- Mount Everest
- Ladakh
- Andes Mountains
- Himalayas
Pathophysiology (Key Exam Concept)
Hypoxia triggers uneven pulmonary vasoconstriction, leading to pulmonary hypertension and capillary stress failure.
Mechanism sequence
- Hypoxia at altitude
- Hypoxic pulmonary vasoconstriction
- Marked pulmonary artery pressure rise
- Regional over-perfusion of some capillaries
- Capillary stress failure → leak
- Protein-rich pulmonary edema
Important characteristics:
- Non-inflammatory
- Normal LV function
- Patchy edema
Hemodynamic Findings
| Parameter | Finding |
|---|---|
| Pulmonary artery pressure | Markedly elevated |
| Pulmonary capillary wedge pressure | Normal |
| Cardiac function | Normal |
| Edema fluid | Protein rich |
Risk Factors
Major risk factors:
• Rapid ascent
• Strenuous exercise
• Previous HAPE episode
• Cold exposure
• Male sex
• Young age
Medical predispositions:
- Pulmonary hypertension susceptibility
- Patent foramen ovale
- Reduced nitric oxide production
Clinical Features
Symptoms usually develop 2–5 days after ascent.
Early symptoms
- Reduced exercise tolerance
- Dyspnea on exertion
- Dry cough
- Fatigue
Progressive symptoms
- Dyspnea at rest
- Tachycardia
- Tachypnea
- Productive cough (pink frothy sputum)
Severe signs
- Cyanosis
- Altered mental status
- Severe hypoxemia
Physical Examination
Typical findings:
- Crackles (initially right middle lobe)
- Tachycardia
- Tachypnea
- Low oxygen saturation
- Mild fever
Imaging
Chest X-ray
Features:
- Patchy alveolar infiltrates
- Often perihilar
- Normal heart size
- Asymmetric edema
CT findings
- Ground glass opacities
- Patchy consolidation
Diagnostic Criteria (Lake Louise HAPE Score)
Diagnosis requires:
Symptoms
- Dyspnea at rest
- Cough
- Weakness
PLUS
Signs
- Crackles
- Central cyanosis
- Tachypnea
- Tachycardia
Management (Emergency)
1. Immediate descent (MOST IMPORTANT)
Descending 500–1000 m often improves symptoms rapidly.
2. Oxygen therapy
Target:
SpO₂ > 90%
3. Pharmacologic therapy
| Drug | Mechanism |
|---|---|
| Nifedipine | Pulmonary vasodilation |
| Tadalafil | PDE-5 inhibitor |
| Sildenafil | ↓ pulmonary pressure |
| Dexamethasone | Adjunct |
Preferred drug
Nifedipine SR 30 mg every 12 hr
4. Portable hyperbaric chamber
Used when descent is not possible.
Example:
- Gamow Bag portable altitude chamber
Prevention
Gradual ascent (most effective)
Rule:
Do not increase sleeping altitude >500 m/day above 3000 m
Add rest day every 3–4 days.
Drug prophylaxis for high-risk individuals
| Drug | Dose |
|---|---|
| Nifedipine SR | 30 mg BD |
| Tadalafil | 10 mg BD |
| Sildenafil | 50 mg TDS |
Important Differentials
| Condition | Key difference |
|---|---|
| Cardiogenic pulmonary edema | Elevated PCWP |
| Pneumonia | Fever, consolidation |
| Pulmonary embolism | Acute pleuritic pain |
10 NEET-SS Exam Pearls
- HAPE is non-cardiogenic pulmonary edema.
- Occurs >2500–3000 m altitude.
- Hypoxic pulmonary vasoconstriction is the primary trigger.
- Pulmonary capillary wedge pressure is normal.
- Chest X-ray shows patchy asymmetric infiltrates with normal heart size.
- Symptoms appear 2–5 days after ascent.
- Immediate descent is the most effective treatment.
- Nifedipine is the first-line drug.
- Oxygen therapy rapidly improves symptoms.
- Prior HAPE episode is the strongest risk factor.
High-Altitude Illness Rapid Revision
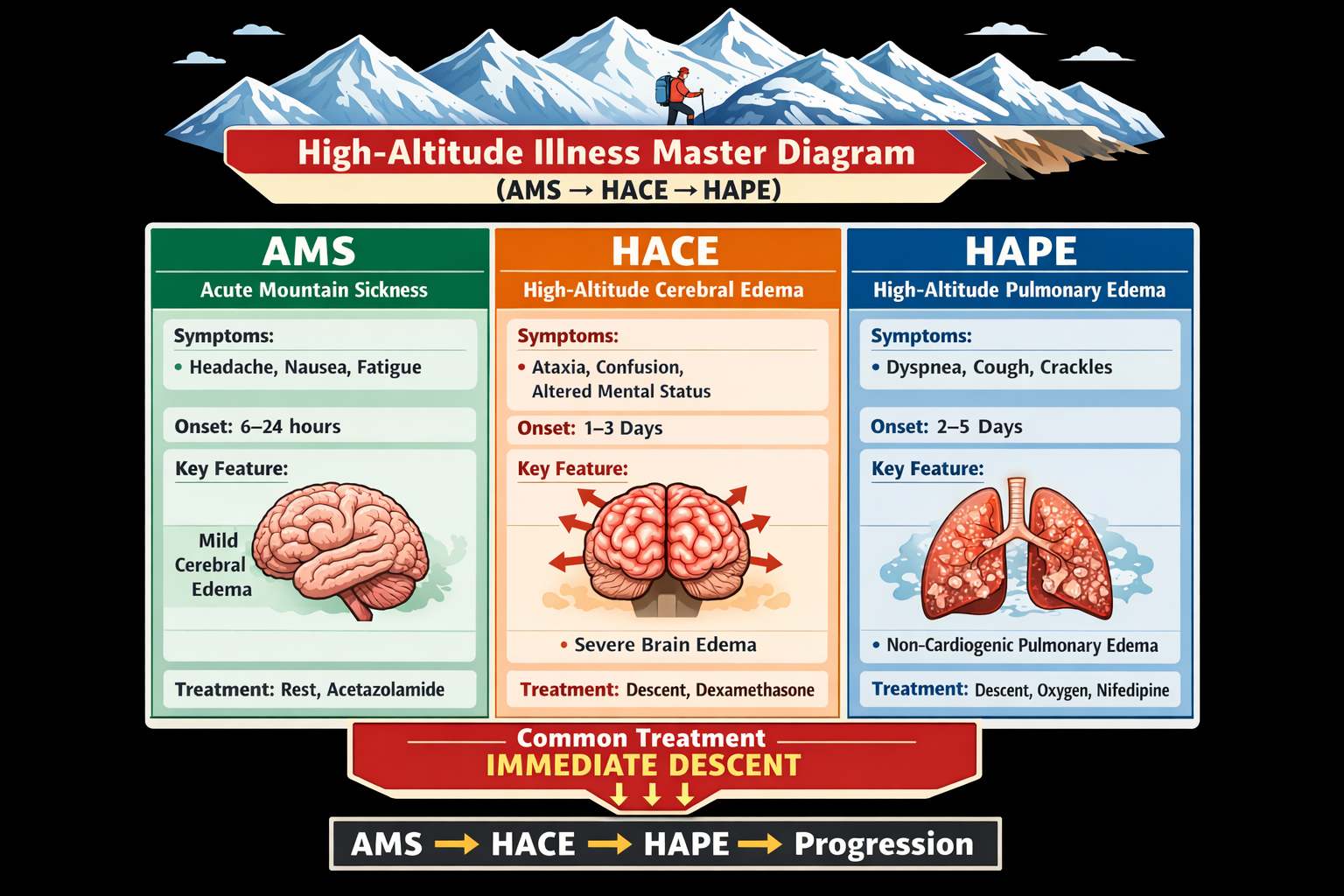
HAPE vs HACE vs AMS (NEET-SS Favorite Table)
| Feature | AMS (Acute Mountain Sickness) | HACE (High-Altitude Cerebral Edema) | HAPE (High-Altitude Pulmonary Edema) |
|---|---|---|---|
| Primary organ involved | Brain (mild cerebral edema) | Brain (severe vasogenic edema) | Lungs (non-cardiogenic pulmonary edema) |
| Altitude threshold | >2500 m | Usually >3500–4000 m | >3000 m |
| Onset after ascent | 6–24 hours | Usually 1–5 days | 2–5 days |
| Pathophysiology | Hypoxia → mild cerebral edema | Hypoxia → blood–brain barrier breakdown → vasogenic edema | Uneven hypoxic pulmonary vasoconstriction → pulmonary hypertension → capillary leak |
| Pulmonary artery pressure | Normal | Normal | Markedly elevated |
| PCWP | Normal | Normal | Normal (non-cardiogenic) |
| Key early symptom | Headache | Severe headache + ataxia | Dyspnea on exertion |
| Major symptoms | Headache, nausea, fatigue, dizziness | Ataxia, confusion, altered consciousness | Dyspnea, cough, exercise intolerance |
| Neurologic signs | None or mild | Ataxia (hallmark), confusion, coma | Usually absent |
| Respiratory signs | Normal lungs | Normal lungs | Crackles, tachypnea, hypoxemia |
| Chest X-ray | Normal | Normal | Patchy infiltrates with normal heart size |
| MRI brain | Usually normal | White-matter vasogenic edema | Not applicable |
| ABG | Mild hypoxemia | Moderate hypoxemia | Severe hypoxemia |
| Most important treatment | Rest ± acetazolamide | Immediate descent + dexamethasone | Immediate descent + oxygen |
| Drug of choice | Acetazolamide | Dexamethasone | Nifedipine |
| Portable chamber | Occasionally used | Often used | Often used |
| Mortality risk | Very low | High if untreated | High if untreated |
| Progression relationship | May precede HACE | Severe progression of AMS | Usually independent |
Key Exam Traps (NEET-SS)
1️⃣ Hallmark of HACE:
👉 Ataxia
2️⃣ Hallmark of HAPE:
👉 Dyspnea with crackles + normal PCWP
3️⃣ Drug prophylaxis differences
| Condition | Drug |
|---|---|
| AMS | Acetazolamide |
| HACE | Dexamethasone |
| HAPE | Nifedipine / Sildenafil |
Rapid Mnemonic
“HEAD–BRAIN–LUNG”
| Disease | Key Feature |
|---|---|
| AMS | Headache |
| HACE | Brain dysfunction (ataxia) |
| HAPE | Lung edema |
5 Super-High-Yield SS Pearls
1️⃣ Ataxia = HACE until proven otherwise.
2️⃣ Normal PCWP distinguishes HAPE from cardiogenic edema.
3️⃣ AMS can progress to HACE but rarely to HAPE.
4️⃣ HAPE chest X-ray shows patchy asymmetric infiltrates.
5️⃣ Immediate descent is the most important treatment in all three.