Diagnosis and management of stress cardiomyopathy (Takotsubo syndrome)
Diagnosis and management of stress cardiomyopathy (Takotsubo syndrome)
TRESS (TAKOTSUBO) CARDIOMYOPATHY – 100 FAQs WITH EXPLANATIONS
BASICS & DEFINITIONS
1. What is Takotsubo cardiomyopathy?
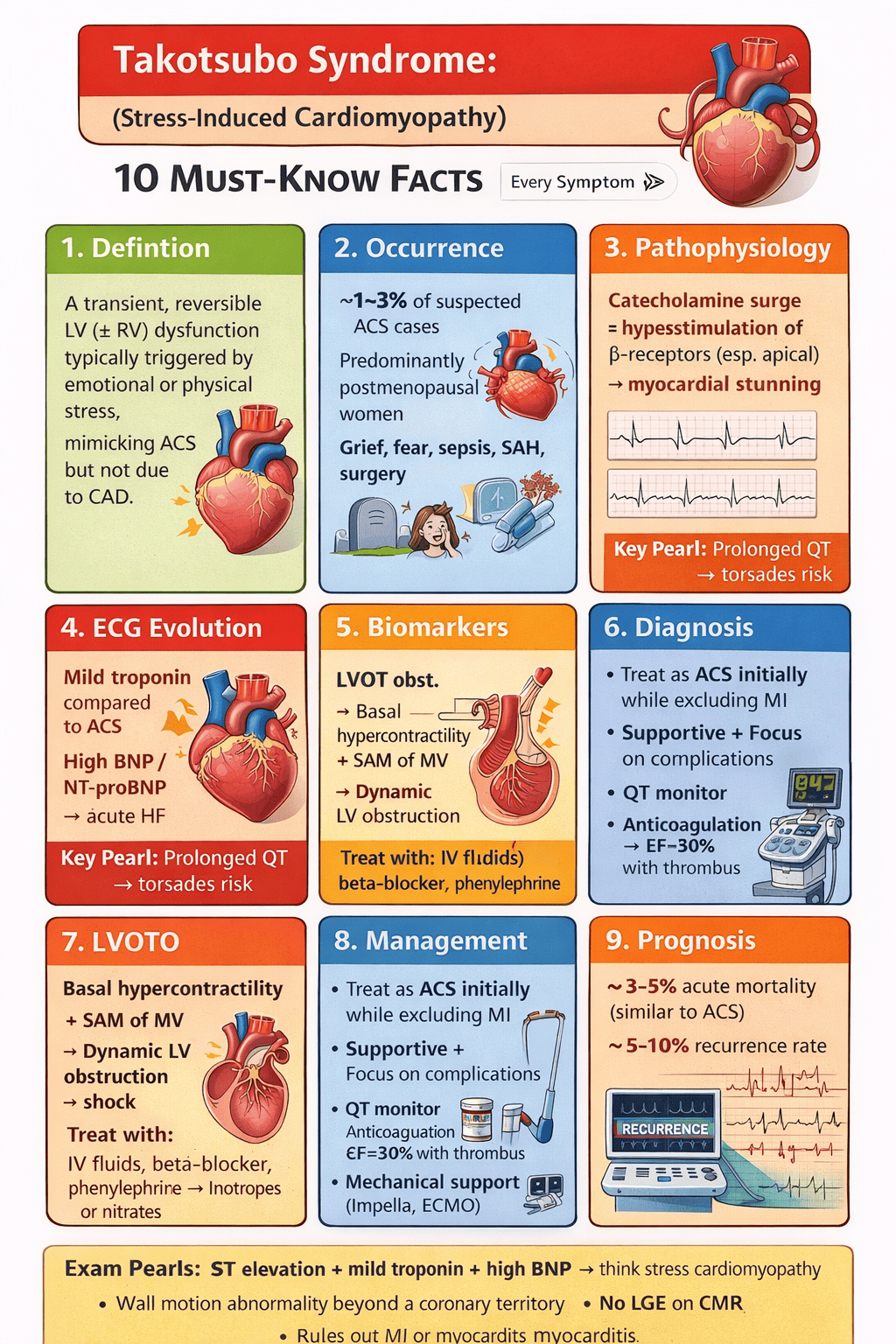
A transient acute heart failure syndrome with reversible LV (± RV) systolic dysfunction, triggered by stress, not explained by obstructive CAD.
2. Why is it called “Takotsubo”?
The LV in systole resembles a Japanese octopus pot (takotsubo) due to apical ballooning.
3. Is Takotsubo a form of myocardial infarction?
No. It mimics ACS clinically but lacks irreversible ischemic necrosis.
4. Is coronary artery disease excluded in Takotsubo?
No. CAD may coexist, but it does not explain the regional dysfunction.
5. Is a stress trigger mandatory for diagnosis?
No. A trigger is common but not required (InterTAK criteria).
EPIDEMIOLOGY
6. Which population is most affected?
Postmenopausal women (~90%).
7. Why are postmenopausal women predisposed?
Loss of estrogen-mediated catecholamine buffering and microvascular protection.
8. How common is Takotsubo among ACS presentations?
~1–3% of suspected ACS cases.
9. Can men develop Takotsubo?
Yes, often triggered by physical stress and associated with worse outcomes.
10. What age group is typical?
Sixth to eighth decade.
TRIGGERS
11. What are emotional triggers?
Grief, fear, anger, financial stress, arguments, bad news.
12. What are physical triggers?
Sepsis, surgery, trauma, stroke, subarachnoid hemorrhage, respiratory failure.
13. Which trigger predicts worse prognosis?
Physical stress triggers.
14. Which neurologic trigger is classically associated?
Subarachnoid hemorrhage.
15. Why do neurologic triggers cause severe Takotsubo?
Massive sympathetic discharge causing catecholamine toxicity.
PATHOPHYSIOLOGY
16. What is the central pathogenic mechanism?
Catecholamine-mediated myocardial stunning.
17. How do catecholamines damage myocardium?
β-receptor overstimulation → calcium overload → oxidative stress → stunning.
18. Why is the apex commonly involved?
Higher β-adrenergic receptor density at the apex.
19. Why does basal Takotsubo occur?
Different receptor distribution and extreme catecholamine states.
20. Is microvascular dysfunction involved?
Yes, transient coronary microvascular spasm contributes.
CLINICAL PRESENTATION
21. Most common presenting symptom?
Acute chest pain.
22. Other common presentations?
Dyspnea, syncope, cardiogenic shock, arrhythmias.
23. Can Takotsubo present without chest pain?
Yes, especially in ICU or neuro-triggered cases.
24. Can Takotsubo cause cardiogenic shock?
Yes (5–10%), due to pump failure or LVOTO.
25. Why is early differentiation from ACS difficult?
Clinical, ECG, and troponin findings overlap.
ECG FEATURES
26. Typical early ECG finding?
ST-segment elevation (often anterior).
27. How does Takotsubo ST elevation differ from STEMI?
Less reciprocal changes, rapid evolution.
28. Typical subacute ECG change?
Deep symmetric T-wave inversion.
29. Late ECG hallmark?
Marked QT prolongation.
30. Why is QT prolongation important?
Predisposes to torsades de pointes.
BIOMARKERS
31. How high is troponin elevation?
Mild to moderate, disproportionate to ECG changes.
32. BNP levels in Takotsubo?
Markedly elevated.
33. Useful diagnostic ratio?
High BNP / troponin ratio.
34. Why is BNP so high?
Acute myocardial stretch and heart failure.
35. Does CK-MB rise significantly?
Usually mild compared to MI.
ECHOCARDIOGRAPHY
36. Key echo feature of Takotsubo?
Regional wall motion abnormality beyond a single coronary territory.
37. Most common variant?
Apical ballooning (~70%).
38. Other variants?
Mid-ventricular, basal (reverse), focal, global.
39. What is LVOTO in Takotsubo?
Dynamic obstruction due to basal hypercontractility.
40. How is LVOTO detected?
Doppler gradient >30 mmHg with SAM of mitral valve.
COMPLICATIONS ON ECHO
41. Why does SAM occur?
Hyperdynamic basal segments pull mitral valve anteriorly.
42. Consequence of LVOTO?
Hypotension, shock, worsening MR.
43. Which echo finding predicts worse prognosis?
RV involvement.
44. Why does RV involvement matter?
Indicates extensive myocardial stunning.
45. When does LV thrombus occur?
With severe apical akinesia and low EF.
CORONARY ANGIOGRAPHY
46. Is angiography mandatory?
Yes, in ACS-like presentations.
47. Typical angiographic finding?
Normal or non-obstructive coronaries.
48. Does obstructive CAD exclude Takotsubo?
No, if wall-motion pattern is inconsistent.
49. Why angiography is critical?
To exclude plaque rupture MI.
50. Can spasm be seen?
Occasionally, but not required for diagnosis.
CARDIAC MRI (CMR)
51. Role of CMR in Takotsubo?
Gold standard for tissue characterization.
52. Key CMR finding?
Myocardial edema.
53. LGE pattern in Takotsubo?
Absent or minimal, non-ischemic.
54. How does CMR differentiate myocarditis?
Myocarditis shows patchy inflammatory LGE.
55. Native T1 and T2 mapping findings?
Both elevated due to diffuse edema.
DIFFERENTIAL DIAGNOSIS
56. Takotsubo vs STEMI – key difference?
Reversibility and lack of infarct LGE.
57. Takotsubo vs myocarditis?
Myocarditis has inflammatory LGE and persistent dysfunction.
58. Takotsubo vs MINOCA?
MINOCA often has ischemic LGE or plaque disruption.
59. Takotsubo vs HOCM with LVOTO?
LVOTO in Takotsubo is transient.
60. Takotsubo vs catecholamine myocarditis?
Myocarditis shows inflammatory fibrosis on CMR.
ACUTE MANAGEMENT – GENERAL
61. Initial management approach?
Treat as ACS until diagnosis confirmed.
62. Role of antiplatelets initially?
Given until MI is excluded.
63. Is thrombolysis indicated?
No, unless STEMI cannot be excluded.
64. Role of ACE inhibitors?
Improve recovery and outcomes.
65. Role of beta-blockers?
Useful after stabilization; benefit for recurrence uncertain.
SHOCK MANAGEMENT
66. First step in Takotsubo shock?
Assess for LVOTO.
67. Why is this step critical?
Management differs completely.
68. Shock with LVOTO – avoid which drugs?
Inotropes, nitrates, aggressive diuresis.
69. Preferred therapy in LVOTO shock?
IV fluids, beta-blockers, phenylephrine.
70. Why phenylephrine?
Pure alpha effect increases afterload without inotropy.
SHOCK WITHOUT LVOTO
71. Mechanism of shock without LVOTO?
Severe global LV systolic dysfunction.
72. Inotropes role here?
Can be used cautiously.
73. Preferred vasopressor?
Norepinephrine.
74. Mechanical support options?
Impella, VA-ECMO in refractory cases.
75. Why IABP is controversial?
Afterload reduction may worsen LVOTO.
ARRHYTHMIAS
76. Most dangerous arrhythmia?
Torsades de pointes.
77. Why torsades occurs?
QT prolongation due to myocardial edema.
78. Management of torsades?
IV magnesium, correction of electrolytes.
79. Are ICDs indicated?
No, unless another indication exists.
80. Duration of telemetry monitoring?
Until QT normalizes and stable.
ANTICOAGULATION
81. When is anticoagulation indicated?
LV thrombus or severe apical akinesia with EF <30%.
82. Duration of anticoagulation?
Until LV function and wall motion recover.
83. DOAC vs warfarin?
Either acceptable; evidence limited.
84. Is prophylactic anticoagulation routine?
No, only in high-risk patients.
85. Risk of embolic stroke?
Low but significant if thrombus present.
PROGNOSIS & FOLLOW-UP
86. Is Takotsubo benign?
No, acute mortality comparable to ACS.
87. In-hospital mortality?
~3–5%.
88. What drives long-term mortality?
Comorbidities, not cardiomyopathy itself.
89. Recurrence rate?
~5–10%.
90. Best follow-up imaging?
Echocardiography at 4–6 weeks.
PREVENTION & LONG-TERM CARE
91. Do beta-blockers prevent recurrence?
Evidence inconsistent.
92. Which drug shows best survival association?
ACE inhibitors / ARBs.
93. Role of psychiatric evaluation?
Important in emotional-triggered cases.
94. Is lifestyle modification relevant?
Yes, stress management reduces recurrence risk.
95. When can HF therapy be stopped?
After documented LV recovery.
EXAM PEARLS
96. High BNP with modest troponin suggests?
Takotsubo cardiomyopathy.
97. Absence of LGE on CMR implies?
No irreversible myocardial injury.
98. Hypotension worsens after inotropes → think?
LVOTO.
99. Basal Takotsubo is linked to?
Neurogenic catecholamine surge.
100. One sentence diagnosis of Takotsubo?
A reversible stress-induced cardiomyopathy mimicking ACS with transient LV dysfunction beyond a single coronary territory.