Windblown Appearance
Windblown Appearance
‘windblown appearance’ is seen in epithelium of which disease?
A. Dermatomyositis
B. DLE
C. Bowen′s disease
D. Morphea

Bowen′s disease – epithelium
Epidermis shows
- Acanthosis
- Elongation and thickening of the rete ridges
- Crowding of keratinocyte.
- Anisocytosis
- Loss of polarity
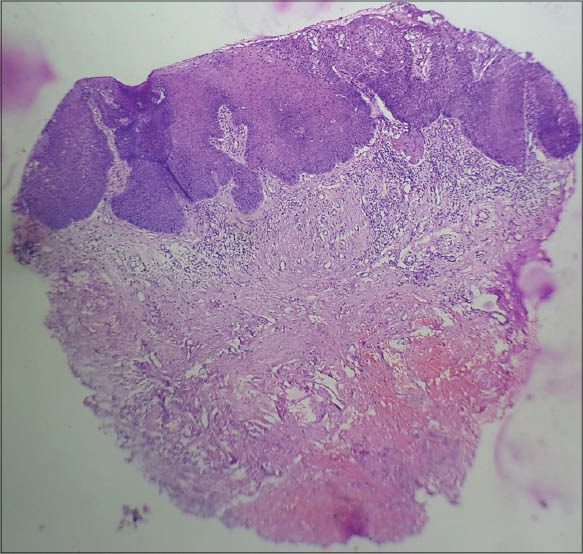
Throughout the epidermis, the cells lie in complete disorder, resulting in a “wind-blown” appearanc
| Windblown Appearance – Bowen′s disease – epithelium | ||
| 1 | Acanthosis | |
| 2 | Elongation and thickening of the rete ridges | |
| 3 | Crowding of keratinocyte. | |
| 4 | Anisocytosis | |
| 5 | Loss of polarity |
Windblown Appearance – Bowen′s disease – epithelium
📌 Key Points:
- Disorderly arrangement of keratinocytes throughout the entire epidermis
- Loss of normal polarity (wind-blown appearance)
- Nuclear atypia and dysplasia at all levels of the epidermis
- Basement membrane remains intact (no invasion)
- Clinically: scaly, erythematous plaque, often mistaken for psoriasis or eczema
1. The “wind-blown” appearance of epidermal cells is a hallmark of which condition?
Seen in Bowen’s disease (SCC in situ), due to disorderly epidermal arrangement.
2. Bowen’s disease is best described as:
Bowen’s disease = SCC in situ, confined to epidermis without basement membrane invasion.
3. Which epidermal layer shows atypia in Bowen’s disease?
Bowen’s disease shows full-thickness epidermal atypia with intact basement membrane.
4. Which is the most specific histological feature of Bowen’s disease?
“Wind-blown” arrangement of keratinocytes is classic for Bowen’s disease.
5. The basement membrane in Bowen’s disease is:
In Bowen’s disease, the basement membrane remains intact, distinguishing it from invasive SCC.
6. Bowen’s disease most commonly affects which age group?
It is typically seen in middle-aged and elderly adults.
7. Which virus has been implicated in genital Bowen’s disease?
HPV-16 is strongly linked to genital Bowen’s disease.
8. Clinical presentation of Bowen’s disease is usually:
Typically presents as a well-demarcated, scaly erythematous plaque.
9. Which of the following is a premalignant condition progressing to invasive SCC?
Bowen’s disease can progress to invasive squamous cell carcinoma.
10. Which of the following sites is most commonly affected in Bowen’s disease?
The lower limbs, especially sun-exposed areas, are common sites.
11. Which of the following is the genital counterpart of Bowen’s disease in men?
Erythroplasia of Queyrat is SCC in situ on glans penis, considered genital Bowen’s disease.
12. Which feature differentiates Bowen’s disease from invasive squamous cell carcinoma?
The basement membrane remains intact in Bowen’s disease, unlike invasive SCC.
13. What is the approximate risk of progression of Bowen’s disease to invasive SCC?
About 3–5% of cases progress to invasive squamous cell carcinoma.
14. Which of the following is NOT a risk factor for Bowen’s disease?
Important risk factors: sunlight, arsenic, HPV, immunosuppression. Vitamin D intake is not linked.
15. Histologically, Bowen’s disease is most often confused with:
Psoriasis may mimic Bowen’s, but lacks full-thickness atypia and wind-blown cells.
16. Which clinical sign suggests Bowen’s disease over psoriasis?
Unlike psoriasis, Bowen’s disease presents as a solitary plaque with irregular surface.
17. Which site is least commonly affected by Bowen’s disease?
The palms and soles are rare sites for Bowen’s disease.
18. The term “Bowenoid papulosis” refers to:
Bowenoid papulosis: HPV-related pigmented papules histologically similar to Bowen’s disease.
19. Which treatment is commonly used for localized Bowen’s disease?
Treatment includes cryotherapy, surgical excision, topical 5-FU or imiquimod.
20. Which immunohistochemical marker supports diagnosis of Bowen’s disease?
p16 is often positive in HPV-related Bowen’s disease.







