Mitral valve repair versus replacement
Mitral Valve Repair vs Replacement — high-yield comparative overview
1. Definitions
- Mitral valve repair (MVr): Surgical correction of native valve (leaflet resection, chordal repair/replacement, annuloplasty ring).
- Mitral valve replacement (MVR): Excision of native valve with implantation of mechanical or bioprosthetic valve.
2. Indications (etiology-driven)
| Etiology | Repair preferred | Replacement preferred |
|---|---|---|
| Degenerative MR (myxomatous, prolapse, flail) | Yes – gold standard (durable, low mortality) | Rare (extensive calcification, failed repair) |
| Ischemic MR | Selected cases (restrictive annuloplasty ± subvalvular repair) | Severe tethering, recurrent MR risk |
| Rheumatic disease | Limited (early disease, pliable leaflets) | Common (calcification, chordal fusion) |
| Endocarditis | If tissue destruction limited | Yes when extensive destruction/abscess |
| Functional MR (HFrEF) | Selected (surgery with CABG) | Rare; high recurrence after repair |
| Congenital anomalies | Often | When anatomy unsuitable |
3. Advantages
Mitral Valve Repair
- Preserves LV geometry and function
- Lower peri-operative mortality
- Better long-term survival
- No lifelong anticoagulation
- Lower risk of thromboembolism, endocarditis
- Superior quality of life
Mitral Valve Replacement
- Predictable elimination of MR
- Technically simpler in hostile anatomy
- Option when repair durability is doubtful
4. Disadvantages
Repair
- Technically demanding; operator-dependent
- Risk of recurrent MR (ischemic/functional MR)
Replacement
- Loss of subvalvular apparatus → LV dysfunction (unless chordal-sparing)
- Anticoagulation required (mechanical)
- Structural valve degeneration (bioprosthesis)
- Higher risk of prosthetic thrombosis, PPM, endocarditis
5. Outcomes (key points)
- Degenerative MR: Repair → lower mortality, better 10–20 yr survival
- Ischemic MR: Replacement reduces recurrent MR; survival similar
- Functional MR: High recurrence after repair; replacement in selected cases
- Rheumatic MR: Replacement often more durable
6. Special considerations
- Age: Young → repair preferred; elderly may tolerate bioprosthetic MVR
- Atrial fibrillation: Concomitant MAZE often with repair
- Anticoagulation contraindication: Repair or bioprosthetic valve
- Surgeon/center expertise: High-volume repair centers matter
7. Guideline-style take-home
Mitral valve repair is the treatment of choice for severe degenerative MR when a durable repair is feasible.
Replacement is reserved for non-repairable anatomy, advanced rheumatic disease, or extensive infective destruction.
1. In severe degenerative MR, the single most important determinant favoring repair over replacement is:
Age <60 years
Absence of atrial fibrillation
Expected durability of repair >95%
Normal LV ejection fraction
Durable repair feasibility is the **key deciding factor**. Guidelines prioritize repair **only when durability is high**, irrespective of age or rhythm.
2. Which pathological feature most strongly predicts failure of mitral valve repair in ischemic MR?
Annular dilatation
Posterior leaflet restriction
LV end-diastolic diameter >55 mm
Severe leaflet tethering (tenting height >10 mm)
Severe tethering reflects advanced LV remodeling → **high recurrence after repair**, hence replacement preferred.
3. Compared with replacement, mitral valve repair improves survival primarily by:
Reducing pulmonary hypertension
Preserving subvalvular-LV interaction
Reducing atrial fibrillation burden
Eliminating regurgitation completely
Repair preserves **chordae-papillary-LV geometry**, preventing postoperative LV dysfunction.
4. Which scenario most strongly mandates mitral valve replacement?
P2 prolapse
Functional MR with CABG
Rheumatic MR with heavy leaflet calcification
Early infective endocarditis
Advanced rheumatic disease causes **irreversible structural distortion**, making repair non-durable.
5. Chordal-sparing during mitral valve replacement primarily prevents:
Paravalvular leak
Prosthetic thrombosis
Patient–prosthesis mismatch
Postoperative LV systolic dysfunction
Loss of chordae disrupts LV mechanics → acute LV failure unless preserved.
6. Which repair component is mandatory in almost all mitral valve repairs?
Leaflet resection
Chordal shortening
Annuloplasty ring
Edge-to-edge stitch
Annuloplasty restores geometry and prevents late annular dilatation → **key durability step**.
7. In infective endocarditis, repair is preferred over replacement when:
Large vegetations are present
Leaflet destruction is limited
Annular abscess exists
Active sepsis persists
Limited destruction allows durable repair and avoids prosthetic infection risk.
8. Why is mitral valve replacement favored in severe functional MR with LV dilation?
Lower operative time
Better reverse remodeling
Improved EF recovery
Lower MR recurrence
Repair fails due to progressive LV tethering → replacement more durable.
9. Which valve choice mandates lifelong anticoagulation?
Bioprosthetic MVR
Mitral repair
Mechanical MVR
Edge-to-edge repair
Mechanical valves require lifelong anticoagulation due to thrombogenicity.
10. Long-term survival advantage of repair over replacement is MOST evident in:
Rheumatic MR
Degenerative MR
Endocarditis
Functional MR
Strongest evidence for repair superiority exists in **degenerative MR**.
11. Which echocardiographic tethering parameter best predicts recurrent MR after restrictive annuloplasty in ischemic MR?
Annular diameter >35 mm
Posterior leaflet angle >30°
Coaptation length <2 mm
Tenting height >10 mm
Among all indices, **tenting height >10 mm** best reflects irreversible LV remodeling → repair failure.
12. In ischemic MR, a posterior leaflet angle >45° implies:
High likelihood of durable repair
Isolated annular pathology
Severe leaflet tethering with high recurrence risk
Better response to edge-to-edge repair
Posterior leaflet angle is a **surrogate of papillary muscle displacement** → recurrence after repair.
13. CTSN trial (severe ischemic MR) showed that compared to replacement, repair resulted in:
Lower mortality at 2 years
Higher rate of recurrent ≥ moderate MR
Better LV reverse remodeling
Lower heart failure hospitalization
CTSN: **Repair had ~58% MR recurrence**, while survival and LV remodeling were similar.
14. In CTSN moderate ischemic MR trial (CABG ± repair), adding repair resulted in:
Improved survival
Significant LV reverse remodeling
Reduced MR but no survival benefit
Reduced stroke rates
Key trap: **less MR ≠ better outcomes**. No survival or remodeling benefit.
15. The most powerful geometric predictor favoring replacement over repair in ischemic MR is:
LVESD >45 mm
Annular dilatation
Reduced coaptation length
Symmetric bileaflet tethering
Symmetric tethering indicates **global LV distortion** → annuloplasty alone fails.
16. Why does restrictive annuloplasty fail in advanced ischemic MR?
Annular redilatation
Ring undersizing
Progressive LV remodeling and papillary displacement
Leaflet calcification
MR is **ventricular disease**, not valvular — the core exam concept.
17. Which echocardiographic finding suggests a potentially repairable ischemic MR?
Tenting height 12 mm
Asymmetric posterior tethering
Posterior leaflet angle 50°
Severe apical papillary displacement
Asymmetric tethering implies **regional ischemia** → better repair durability.
18. A patient with ischemic MR has tenting area 3.0 cm². Best surgical strategy?
Isolated annuloplasty
Edge-to-edge repair
Repair + CABG
Chordal-sparing replacement
Tenting area >2.5 cm² → **repair failure almost certain**.
19. Subvalvular procedures (papillary relocation) in ischemic MR aim to:
Reduce annular size
Increase leaflet tissue
Reduce leaflet tethering forces
Improve atrial compliance
Addresses the **ventricular component** of ischemic MR.
20. Which factor MOST predicts survival benefit after mitral intervention in ischemic MR?
Elimination of MR
Type of surgery
Valve prosthesis choice
Underlying LV function
Survival is **LV-driven**, not valve-driven — classic NEET-SS trap.
21. Which ischemic MR phenotype benefits LEAST from repair?
Inferior MI with posterior tethering
Localized papillary displacement
Global LV dilation with symmetric tethering
Viable myocardium
Global cardiomyopathy = **replacement territory**.
22. Which CTSN conclusion is most commonly tested incorrectly?
Repair has higher MR recurrence
Replacement preserves LV function if chordal-sparing
Mortality similar between groups
Repair improves survival
**Repair does NOT improve survival** — classic exam trap.
23. The concept that ischemic MR is a ventricular disease explains failure of:
Chordal preservation
Annuloplasty alone
Valve replacement
CABG
Annulus is not the primary pathology.
24. Best echocardiographic cutoff suggesting non-durable repair:
Coaptation depth 6 mm
Posterior leaflet length 15 mm
Tenting area >2.5 cm²
Annular diameter 32 mm
Tenting area integrates **height + area** → strongest predictor.
25. In ischemic MR, which surgical principle improves durability of repair?
Smaller annuloplasty ring
Anterior leaflet resection
Edge-to-edge alone
Adding subvalvular repair
Treat **ventricle + valve**, not valve alone.
26. Which parameter is LEAST useful in deciding repair vs replacement?
Tenting height
Posterior leaflet angle
LV geometry
Left atrial size
Decision is **ventricular geometry–driven**, not atrial.
27. Why does replacement not worsen LV function when chordal-sparing?
Improved preload
Reduced afterload
Preserved LV-papillary coupling
Elimination of MR
Chordae are **LV functional units**, not valve remnants.
28. In severe ischemic MR with EF 25%, best surgical approach?
Repair alone
Repair + CABG
Edge-to-edge repair
Chordal-sparing replacement
Low EF + severe tethering → **replacement safer and durable**.
29. Which statement about ischemic MR is TRUE?
Severity correlates with annular size
Severity correlates with LV remodeling
Repair corrects the primary pathology
Eliminating MR reverses cardiomyopathy
Ischemic MR mirrors **ventricular disease severity**.
30. Ultimate exam takeaway from CTSN trials:
Always repair ischemic MR
Always replace ischemic MR
MR elimination improves survival
Patient selection based on LV geometry is critical
**Geometry > valve** — the single most tested concept.
50 ultra-hard ONE-LINER traps for SS final-week revision, strictly centered on
Ischemic MR – Repair vs Replacement (Algorithm-driven thinking)
These are statement-based traps examiners love — short, sharp, and concept-loaded.
🔥 50 Ultra-Hard Ischemic MR One-Liners (SS Level)
- Ischemic MR is a ventricular disease, not a valvular disease.
- Severity of ischemic MR correlates better with LV remodeling than annular size.
- Tenting height >10 mm predicts repair failure more strongly than MR grade.
- Symmetric bileaflet tethering favors replacement over repair.
- Restrictive annuloplasty fails because it does not address papillary displacement.
- Posterior leaflet angle >45° is a surrogate of irreversible LV geometry.
- In ischemic MR, eliminating MR does not guarantee survival benefit.
- CTSN trial: repair increases MR recurrence without improving mortality.
- Chordal-sparing replacement preserves LV function better than non-sparing repair failure.
- Tenting area >2.5 cm² predicts non-durable repair irrespective of EF.
- Annular dilatation alone is rarely the primary driver of ischemic MR.
- Asymmetric tethering implies regional ischemia and better repair durability.
- Global LV dilatation implies replacement territory, not complex repair.
- MR recurrence after repair reflects progressive LV remodeling, not surgical error.
- CTSN moderate MR trial: less MR ≠ better outcomes.
- Repair improves MR severity, not prognosis, in advanced ischemic cardiomyopathy.
- Subvalvular procedures target the ventricular mechanism, not the valve.
- Papillary muscle displacement is the anatomical substrate of ischemic MR.
- Repair durability depends more on LV geometry than leaflet quality.
- EF <30% + severe tethering → replacement safer than repair.
- Annuloplasty ring undersizing cannot overcome symmetric tethering.
- LV sphericity index predicts repair failure better than MR jet area.
- Edge-to-edge repair does not correct ventricular pathology.
- Replacement does not worsen EF when chordae are preserved.
- Mitral repair success is geometry-dependent, not technique-dependent.
- Ischemic MR recurrence after repair is predictable, not random.
- Posterior leaflet restriction is more prognostically important than anterior prolapse.
- Repair is favored when ischemic MR is regional rather than global.
- CABG alone may reduce MR only if myocardium is viable.
- LV reverse remodeling determines outcome more than MR elimination.
- Replacement offers durability, not necessarily survival advantage.
- Ischemic MR severity fluctuates with loading conditions.
- MR reduction without LV recovery does not improve HF outcomes.
- Valve intervention cannot reverse cardiomyopathy.
- CTSN trials refuted the concept that repair is always superior.
- Mitral valve choice does not override LV disease biology.
- Tenting indices integrate papillary position + LV shape.
- Repair failure is highest in symmetric tethering phenotypes.
- Annuloplasty treats the annulus, not the ventricle.
- Replacement treats MR but does not treat LV dysfunction.
- Durable repair requires favorable ventricular geometry.
- Severe ischemic MR is a marker of advanced LV disease.
- MR recurrence after repair predicts heart failure hospitalization.
- LV viability, not MR grade, predicts postoperative recovery.
- Repair in severe tethering is anatomically optimistic but biologically flawed.
- Replacement is preferred when repair durability is doubtful.
- Ischemic MR management is patient-selection driven, not procedure-driven.
- Geometry-based algorithms outperform symptom-based decisions.
- CTSN’s biggest message: stop treating ischemic MR like degenerative MR.
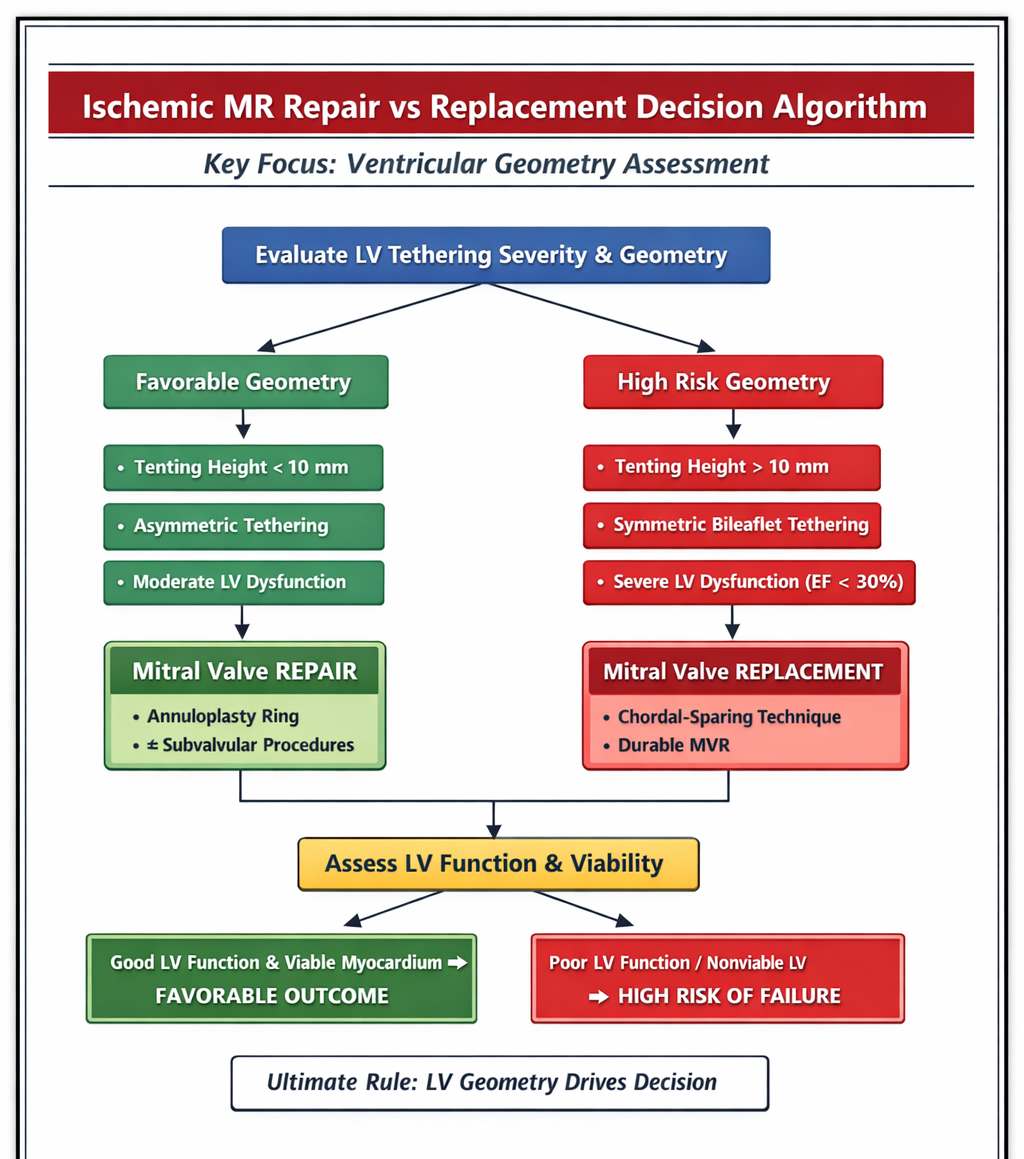
- Ultimate SS rule:
LV geometry decides — the valve only follows.